Herpes Zoster (HZ), also known as shingles or “cacar api”, is the reactivation of latent varicella-zoster virus (VZV) in sensory ganglia, following a prior varicella (chickenpox) infection.
Shingles most commonly reactivates in elderly individuals or those with compromised immunity.
Recognizing shingles “kenali cacar api” early can significantly support healing, as this condition is often overlooked despite its potentially serious impact—especially in vulnerable populations.
Epidemiology
- The incidence of shingles increases significantly in individuals over 50 years of age.
- Approximately 20–30% of the general population will experience shingles at least once in their lifetime.
- Higher risk is observed in patients with HIV, malignancies, or those undergoing immunosuppressive therapy.
Clinical Manifestations
- Prodromal phase: Neuropathic pain (burning, stabbing), often accompanied by malaise and low-grade fever.
- Rash: Appears within 1–5 days as unilateral papulovesicular lesions along a dermatome—commonly thoracic, ophthalmic, or sacral. Duration is 2–4 weeks, with crusting typically within 7–10 days.
- Acute phase: Progression from papules → vesicles → pustules → crusts.
Recognize shingles by its hallmark signs: intense localized pain followed by a unilateral rash.
Clinical variants include:
1. Herpes Zoster Ophthalmicus
- Herpes Zoster “kenali cacar api” that involves the first branch (nasociliary nerve) of the trigeminal nerve (cranial nerve V), which supplies the eye and surrounding areas.
- Key characteristics of Herpes Zoster Ophthalmicus:
- Prodromal symptoms: pain, tingling, or burning sensation around the forehead, upper eyelid, and tip of the nose (dermatomal area V1)
- Unilateral vesicular rash on the forehead, upper eyelid, and upper part of the nose
- Hutchinson’s sign: presence of lesions on the tip of the nose, indicating nasociliary nerve involvement and increased risk of ocular complications
- Ocular symptoms: red eye, photophobia, blurred vision, excessive tearing (epiphora), and eye pain
2. Herpes Zoster Oticus (Ramsay Hunt Syndrome)
- A form of Herpes Zoster caused by reactivation of varicella-zoster virus in the geniculate ganglion of the facial nerve (cranial nerve VII), which innervates the face and ear.
- Key characteristics of Ramsay Hunt Syndrome:
- Severe ear pain (otalgia), often the initial symptom
- Vesicular rash inside the ear canal, on the auricle, or the posterior oral cavity (palate and pharynx)
- Peripheral facial paralysis (similar to Bell’s palsy) → facial asymmetry, difficulty smiling or raising eyebrows
- Hearing loss and/or tinnitus
- Vertigo or balance disturbances
- Sometimes accompanied by systemic symptoms such as fever, fatigue, and loss of appetite
3. Zoster Sine Herpete
- Zoster sine herpete is an atypical form of Herpes Zoster (shingles) that occurs without the appearance of a rash or skin lesions, but still presents with characteristic neuropathic pain on one side of the body along a dermatomal distribution.
- Key characteristics of Zoster Sine Herpete:
- Sharp, burning, or stabbing unilateral pain, similar to typical Herpes Zoster
- No rash or vesicular lesions present on the skin
- Commonly affects the chest, face, or back
- Often misdiagnosed as other forms of neuralgia, musculoskeletal pain, or internal organ disorders
- May still progress to postherpetic neuralgia (PHN) even without skin symptoms
Diagnosis
- Shingles “kenali cacar api” is primarily diagnosed clinically based on dermatomal distribution and lesion characteristics.
- Supporting investigations (if needed):
- VZV PCR from vesicular fluid (gold standard)
- Tzanck smear (nonspecific)
- Serologic testing for atypical cases
Management
- Antivirals
- Acyclovir 800 mg five times daily for 7–10 days
- Valacyclovir 1000 mg three times daily for 7 days
- Famciclovir 500 mg three times daily for 7 days
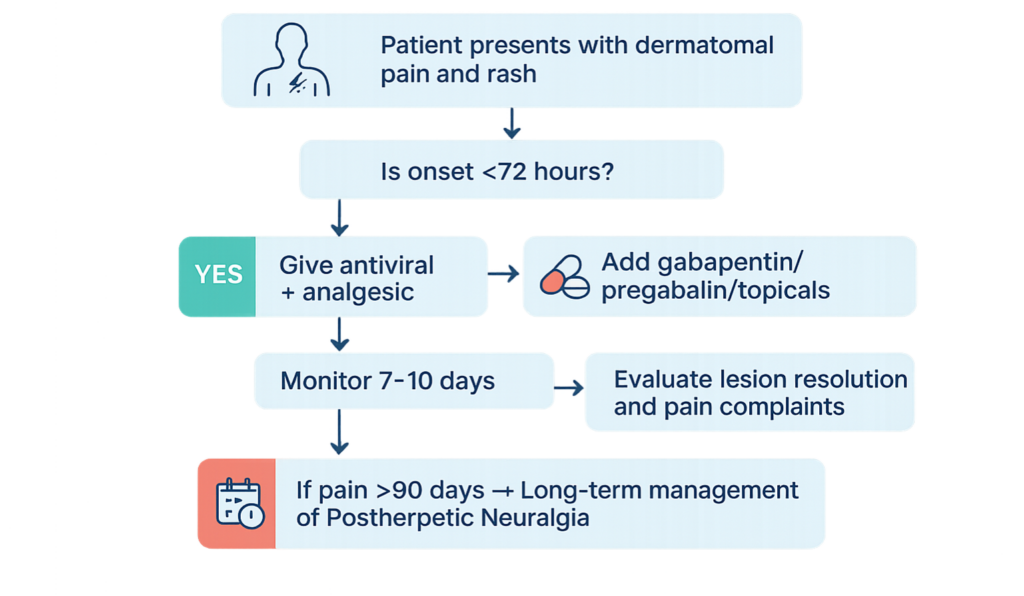
Maximal effectiveness when initiated within 72 hours of rash onset—reducing lesion duration and risk of postherpetic neuralgia (PHN).
- Analgesics
- Mild pain: paracetamol, NSAIDs
- Severe pain or PHN: gabapentin, pregabalin, amitriptyline
- Topical agents: 5% lidocaine patch, capsaicin
- Interventions: nerve block, TENS (Transcutaneous Electrical Nerve Stimulation)
- Oral corticosteroids
- Methylprednisolone (for severe cases, in combination with antivirals)
- Goal: reduce inflammation and risk of PHN
- Antibiotics
If there is secondary bacterial infection (e.g., cellulitis, impetigo)
Prevention
- Balanced nutrition
- Regular physical activity (at least 150 minutes/week)
- Adequate sleep (7–8 hours/day)
- Smoking cessation
- Routine health screenings for early risk detection “kenali cacar api”
- Shingles vaccination: one or two doses depending on vaccine type
Recognize shingles “kenali cacar api” as a vaccine-preventable disease, especially in older adults or those with chronic illness. Recommended for:
- All individuals aged ≥50 years
- Those with a history of HZ or comorbidities
- Immunocompromised patients (based on vaccine type)
Complications
- Postherpetic Neuralgia (PHN): Persistent pain lasting >90 days, especially in the elderly
- Secondary bacterial infection
- Herpes zoster ophthalmicus (involving the first branch of the trigeminal nerve), risk of keratitis or vision loss
- Ramsay Hunt Syndrome (geniculate ganglion involvement), resulting in facial paralysis and auricular vesicles
Management Algorithm
References
- Gagliardi AMZ et al. Vaccines for preventing herpes zoster in older adults. Cochrane Database. 2019.
- Indonesian Dermatology Association. Herpes Zoster Clinical Practice Guidelines. 2023.
- Strezova A, et al. Open Forum Infect Dis. 2022;9(10):ofac485
- CDC. Shingles vaccine recommendations. 2024
- Patil A, Goldust M, Wollina U. Viruses. 2022;14(2):192.
- PAPDI. Adult Immunization Schedule. 2025.
About Docquity
If you need more confidence and insights to boost careers in healthcare, expanding the network to other healthcare professionals to practice peer-to-peer learning might be the answer. One way to do it is by joining a social platform for healthcare professionals, such as Docquity.
Docquity is an AI-based state-of-the-art private & secure continual learning network of verified doctors, bringing you real-time knowledge from thousands of doctors worldwide. Today, Docquity has over 400,000 doctors spread across six countries in Asia.
Meet experts and trusted peers across Asia where you can safely discuss clinical cases, get up-to-date insights from webinars and research journals, and earn CME/CPD credits through certified courses from Docquity Academy. All with the ease of a mobile app available on Android & iOS platforms!






