
Sheehan syndrome, a rare form of hypopituitarism resulting from pituitary gland necrosis following postpartum hemorrhage, poses a significant risk of maternal morbidity and mortality, particularly in regions with inadequate obstetric care. Conversely, it often goes unnoticed in developed countries due to its infrequent occurrence. The case presented involves a 66-year-old woman diagnosed with Sheehan syndrome more than thirty years after her last delivery, which was complicated by postpartum hemorrhage. Despite displaying various symptoms and signs indicative of pituitary hormonal deficiencies, a diagnosis had not been established previously. Comprehensive laboratory analysis revealed a pituitary axis deficiency and cranial imaging showed an empty Sella turcica. Hormonal replacement therapy effectively addressed impairments related to general energy levels, physical capacity, temperature regulation, skin characteristics, and sexual function. Additionally, it mitigated cardiovascular and osteoporosis risks and, critically, prevented a potential life-threatening adrenal crisis.
This report underscores the subtle manifestations of Sheehan syndrome, aiming to assist clinicians in promptly diagnosing the condition, even in developed nations like Portugal, where it should be recognized as a potential cause of hypopituitarism.
Introduction
Hypopituitarism arises from a complete or partial deficiency in pituitary hormones [1]. Sheehan syndrome, a rare cause of hypopituitarism, is marked by the necrosis of the pituitary gland following postpartum hemorrhage. This condition remains relevant in developing countries due to insufficient obstetrical care, leading to maternal morbidity and mortality [2]. Despite being less common in developed nations, a recent retrospective analysis from Iceland indicates an estimated prevalence of 5.1 per 100,000 women [3].
Patients with Sheehan syndrome often have a history of blood transfusions, hysterectomy, and ICU admission following significant postpartum hemorrhage, with no direct correlation between the hemorrhage extent and clinical severity [4]. A retrospective study involving 114 patients revealed a diagnostic delay averaging 19.7 years, attributed to the presentation of nonspecific complaints in a high proportion of affected women [6]. Sheehan syndrome induces secondary adrenal insufficiency, resulting in a selective adrenocorticotropic hormone (ACTH) deficiency, while the renin-angiotensin-aldosterone axis remains intact [7]. Although clinically evident arginine-vasopressin deficiency is rare, around 30% of patients may exhibit partial deficiency based on a water deprivation test [8].
Patients with Sheehan syndrome are often asymptomatic or present with nonspecific symptoms until a stressful event triggers the clinical manifestation. Approximately 55% of patients experience panhypopituitarism. In cases of partial hypopituitarism, growth hormone (GH) and gonadotropins (follicle-stimulating hormone (FSH) and luteinizing hormone (LH)) are commonly affected, followed by thyroid-stimulating hormone (TSH), ACTH, and prolactin [6]. A retrospective study of 60 patients identified asthenia and adynamia in 85%, failure to resume menses in 73%, loss of axillary and pubic hair in 67%, and failure to breastfeed postpartum in 65% of patients as the most commonly reported symptoms [7]. Physical examination findings included decreased or absent pubic or axillary hair in 93%, dry skin in 82%, and pallor in 70%, along with other manifestations such as vaginal atrophy, slow reflexes, mammary gland atrophy, cognitive changes, and myxedema.
Magnetic Resonance Imaging (MRI) is the most sensitive method for evaluating the hypothalamus-pituitary region, revealing an empty Sella turcica of normal size as a characteristic finding in Sheehan syndrome [8]. Given the oftensubtle nature of hypopituitarism, screening appropriate patients is crucial to prevent long-term morbidity, despite its rarity in developed countries, as recent studies suggest that its prevalence may be underestimated [2].
Case Presentation (1)
1. Patient Presentation and Initial Treatment
- A 66-year-old woman with a history of osteoporosis and dyslipidemia was admitted for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia with hypoxemic respiratory failure.
- Started on a daily dose of 6 mg dexamethasone and 35% inspired oxygen.
- Positive clinical evolution; transitioned to room air after five days.
2. Physical Examination Findings
Figure 1: Picture of the patient’s face
(The picture of the patient’s face shows pale skin but a reddish eye mucosa. A marked wrinkling around the eyes and forehead is evident. Dry and weak hair is also partially seen. These findings raised concerns about cortisol and thyroid hormone deficiencies.)

Figure 2: Picture of the patient’s legs
(The picture of the patient’s legs shows the absence of hair. This finding suggested that androgen deficiency due to secondary adrenal insufficiency, as well as hypothyroidism and hypogonadism, could be present.)
- Generalized skin paleness without mucosal discoloration, indicating true hypopigmentation (Figure 1).
- Dry skin, marked wrinkling around the mouth and eyes, thin hair, and absence of axillary and pubic hair (Figure 2).
- Slow movements, preserved muscle strength, vaginal dryness, and atrophy.
- Normal neurological exam, blood pressure, cardiac frequency, and body temperature.
3. Patient’s Medical History
- Long-standing asthenia, cold sensitivity, hot flashes, vaginal dryness, and dyspareunia.
- Stable weight, difficulty tanning, and no lactation since 1990 delivery.
- Obstetric history includes two miscarriages and postpartum complications in 1990.
- Intense headaches and asthenia postpartum; amenorrhea since then.
4. Laboratory and Radiology Studies
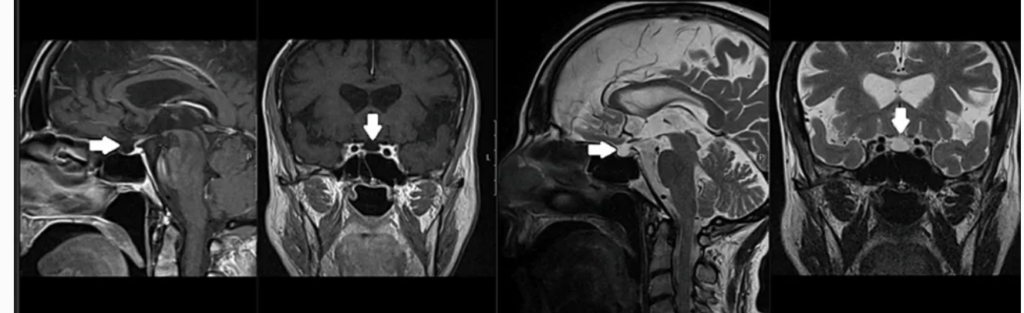
Figure 3: Cranial MRI images
(Cranial MRI of the patient showing an empty Sella turcica (arrows) with pituitary tissue compressed against the sellar floor with lateral stalk deviation)
- Previous analysis revealed low free T4, normal TSH, and negative anti-peroxidase antibodies.
- The new panel shows low free T4, free T3, and reduced FSH/LH, indicating central hypothyroidism and hypogonadism.
- Cranial MRI reveals normal-sized Sella turcica with pituitary parenchyma compressed against the sellar floor (Figure 3).
5. Diagnosis and Treatment Initiation
- Suggestive of Sheehan syndrome due to pituitary ischemia postpartum.
- Levothyroxine supplementation started (1.6 mcg/kg).
- Dexamethasone prevents adrenal crisis; transitioned to oral hydrocortisone.
- Discharged home with ongoing treatment.
6. Follow-up and Clinical Improvement
- Four months post-discharge, progressive improvement was reported: more energy, strength, and faster thinking.
- Stable weight, normal blood pressure, stress dose, and emergency corticoid administration were discussed.
- Pituitary hormonal analysis shows cortisol serum level and confirmed secondary adrenal insufficiency.
7. Hormonal Analysis and Panhypopituitarism Confirmation
Table 1: Laboratory results of pituitary hormone and other relevant tests
*Blood samples were drawn 18 hours after the suspension of hydrocortisone therapy. **On levothyroxine 0.05 mg/day.
- Cortisol level after 18-hour hydrocortisone suspension: 4.49 ug/dL.
- Cosyntropin stimulation test confirms secondary adrenal insufficiency (cortisol level: 8.21 ug/dL after 60 minutes).
- Thyroid function normalized with 50 mcg daily levothyroxine.
- Suppressed FSH/LH, low age-adjusted IGF-1, normal-low prolactin; indicative of panhypopituitarism (Table 1).
8. Further Assessments and Referrals
- Hydroelectrolytic balance, lipid, and glycemic profiles were checked.
- Bone density scan ordered.
- Gynecological appointment for managing vaginal atrophy and sexual complaints.
Discussion
The precise mechanism behind the development of Sheehan syndrome remains incompletely understood. In normal pregnancy, the pituitary gland undergoes enlargement due to the hyperplasia of lactotroph cells stimulated by estrogen [6,8]. This heightened vascularity makes the gland particularly susceptible to changes in arterial pressure [7]. The anterior pituitary, supplied by a low-pressure dense capillary network, becomes even more prone to ischemic events. In cases of severe hypotension resulting from significant postpartum hemorrhage, the pituitary may undergo ischemic necrosis. While hypotheses involving autoimmunity and coagulopathy have been proposed, their specific roles remain unclear [8].
Clinically, individuals with Sheehan syndrome often present with a combination of multiple hormonal deficiencies, each contributing to a distinct set of symptoms. Some manifestations are linked to specific hormones, while others result from various shortcomings. For instance, low libido, hot flashes, infertility, and vaginal dryness are associated with deficiencies in follicle-stimulating hormone (FSH) and luteinizing hormone (LH). In contrast, cold intolerance is related to thyroid-stimulating hormone (TSH). Pallor, dry skin, thinning hair, and loss of body hair are consequences of deficiencies in adrenocorticotropic hormone (ACTH), FSH, and LH. Asthenia, a predominant symptom, is attributed to the concurrent deficiencies of ACTH, TSH, FSH, LH, and growth hormone (GH) [1,2].
Testing for the hypothalamic-pituitary-adrenal (HPA) axis should occur at least 18-24 hours after the last hydrocortisone dose. A cortisol level below three ug/dL indicates adrenal insufficiency, while above 15 ug/dL rules out this diagnosis. When cortisol values fall between 3 and 15 ug/dL, a confirmatory test is advisable, with the cosyntropin stimulation test being the most commonly employed method. This test involves administering 0.25 mg of cosyntropin and measuring serum cortisol levels 60 minutes later; a result equal to or exceeding 18 ug/dL is considered normal [1,4].
Evaluation of central hypothyroidism involves assessing free T4 and TSH levels. A free T4 level below the reference range, in conjunction with a low, normal, or mildly elevated TSH in the context of pituitary disease, typically confirms the diagnosis unless the patient is severely ill [7]. In this case, the acute illness might influence thyroid function tests during hospital admission. However, a previous analysis confirmed a low free T4 of 0.30 ng/dL (reference range: 0.89-1.76 ng/dL) and a normal TSH of 3.37 uUI/mL (reference range: 0.55-4.78 uUI/mL), both of which were consistent with central hypothyroidism [5,6].
In postmenopausal women, the absence of elevated serum FSH and LH levels alone is sufficient for diagnosing gonadotropic dysfunction [1]. In this case, the patient, in the postmenopausal phase, exhibited low levels of both FSH and LH, having been amenorrheic since her last delivery at 34 years of age. In patients with hypothalamic-pituitary disease presenting with three or more hormone deficiencies, a serum IGF-1 level below the reference range indicates a GH deficiency with over a 97% likelihood, eliminating the need for a GH stimulation test [7,1]. In this scenario, the patient’s IGF-1 level of 48.30 ng/mL, falling below the reference range, confirmed a GH deficiency, aligning with recent European analyses setting an IGF-1 reference value of 58.95 to 193.70 ng/mL for individuals aged 66 to 70 years [1,2].
Prolactin deficiency, solely resulting in the inability to lactate after delivery, can be identified through various tests, with some authors suggesting the TRH stimulation test as the most sensitive [9]. In this case, the patient’s inability to lactate further indicated a prolactin deficiency. Although arginine-vasopressin deficiency is a rare manifestation of Sheehan syndrome, the patient displayed normal plasma osmolarity, serum sodium, and 24-hour urinary volume. The MRI findings revealed the characteristic aspects of an empty Sella turcica, with a diagnostic delay of 32 years, longer than previously reported in the literature [6,8].
Replacement therapy for hypopituitarism necessitates a personalized approach with frequent dose adjustments. Standard glucocorticoid doses usually comprise 10-20 mg of hydrocortisone daily, administered in divided doses, with the highest dose in the morning to replicate circadian cortisol secretion. A higher dose is crucial to prevent an adrenal crisis during stressful situations. Thyroid hormone supplementation aims to maintain a free T4 level close to the upper limit of the reference range. For females with a uterus, estrogen and progesterone combination therapy is recommended until reaching the mean age of natural menopause to reduce cardiovascular disease and mortality risks [1].
Growth hormone supplementation, although advised for improved body composition and lipoprotein metabolism, presents discomfort with daily subcutaneous injections and common adverse effects such as edema, arthralgia, and myalgia. Prolactin replacement is currently unavailable [7,3].
The patient lived for over 30 years with severe hormonal deficiencies impacting various aspects of her health. She reported diminished general energy, physical capacity, temperature regulation, skin characteristics, and sexual life. The absence of natural female estrogen protection until menopause heightened her vulnerability to cardiovascular events and osteoporosis. Thyroid and growth hormone deficiencies contribute to hyperlipidemia, insulin resistance, premature atherosclerosis, and cardiac dysfunction [1]. The risk of adrenal crisis during stressful situations was significantly elevated due to adrenal insufficiency, though thankfully, she had not experienced severe illness or required surgical intervention during this period.
Conclusion
In this case report, we present an instance of a rare clinical syndrome that went unrecognized for over three decades. A comprehensive clinical history and physical examination identified numerous manifestations of hormonal deficiencies and subsequently confirmed them through laboratory analysis. Cranial imaging further unveiled the extent of pituitary gland destruction. The objective of this report is to underscore the subtle indications of Sheehan syndrome, urging clinicians to consider it as a potential cause of hypopituitarism, even in developed countries like Portugal, where awareness of this condition may be lacking. Timely recognition holds the potential to significantly enhance the quality of life for affected individuals and prevent life-threatening complications stemming from severe hormonal deficiencies.
Reference
- Vasconcelos A, Pinto Ribeiro R, Claúdio Ferreira P, et al. (February 04, 2024) A Case Report of Sheehan Syndrome: A Rare Cause of Hypopituitarism. Cureus 16(2): e53544. doi:10.7759/cureus.53544
- Fleseriu M, Hashim IA, Karavitaki N, Melmed S, Murad MH, Salvatori R, Samuels MH: Hormonal replacement in hypopituitarism in adults: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016, 101:3888-921. 10.1210/jc.2016-2118
- Kovacs K: Sheehan syndrome. Lancet. 2003, 361:520-2. 10.1016/S0140-6736(03)12490-7
- Kristjansdottir HL, Bodvarsdottir SP, Sigurjonsdottir HA: Sheehan’s syndrome in modern times: a nationwide retrospective study in Iceland. Eur J Endocrinol. 2011, 164:349-54. 10.1530/EJE-10-1004
- Ramiandrasoa C, Castinetti F, Raingeard I, Fenichel P, Chabre O, Brue T, Courbière B: Delayed diagnosis of Sheehan’s syndrome in a developed country: a retrospective cohort study. Eur J Endocrinol. 2013, 169:431-8. 10.1530/EJE-13-0279
- Dash RJ, Gupta V, Suri S: Sheehan’s syndrome: clinical profile, pituitary hormone responses and computed sellar tomography. Aust N Z J Med. 1993, 23:26-31. 10.1111/j.1445-5994. 1993.tb00533.x
- Diri H, Tanriverdi F, Karaca Z, et al.: Extensive investigation of 114 patients with Sheehan’s syndrome: a continuing disorder. Eur J Endocrinol. 2014, 171:311-8. 10.1530/EJE-14-0244
- Melmed S, Koenig R, Rosen CJ, Auchus RJ, Goldfine AB: Williams Textbook Of Endocrinology 14th Edition. Elsevier, Amsterdam, Netherlands; 2019.
About Docquity
If you need more confidence and insights to boost careers in healthcare, expanding the network to other healthcare professionals to practice peer-to-peer learning might be the answer. One way to do it is by joining a social platform for healthcare professionals, such as Docquity.
Docquity is an AI-based state-of-the-art private & secure continual learning network of verified doctors, bringing you real-time knowledge from thousands of doctors worldwide. Today, Docquity has over 400,000 doctors spread across six countries in Asia. Meet experts and trusted peers across Asia where you can safely discuss clinical cases, get up-to-date insights from webinars and research journals, and earn CME/CPD credits through certified courses from Docquity Academy. All with the ease of a mobile app available on Android & iOS platforms!






