
Graves’ disease is an autoimmune disorder that can cause hyperthyroidism, an overactive thyroid gland. The thyroid gland is a small, butterfly-shaped gland located in the front of the neck, which produces hormones that regulate the body’s energy use and affect many organs, including the heart 2.
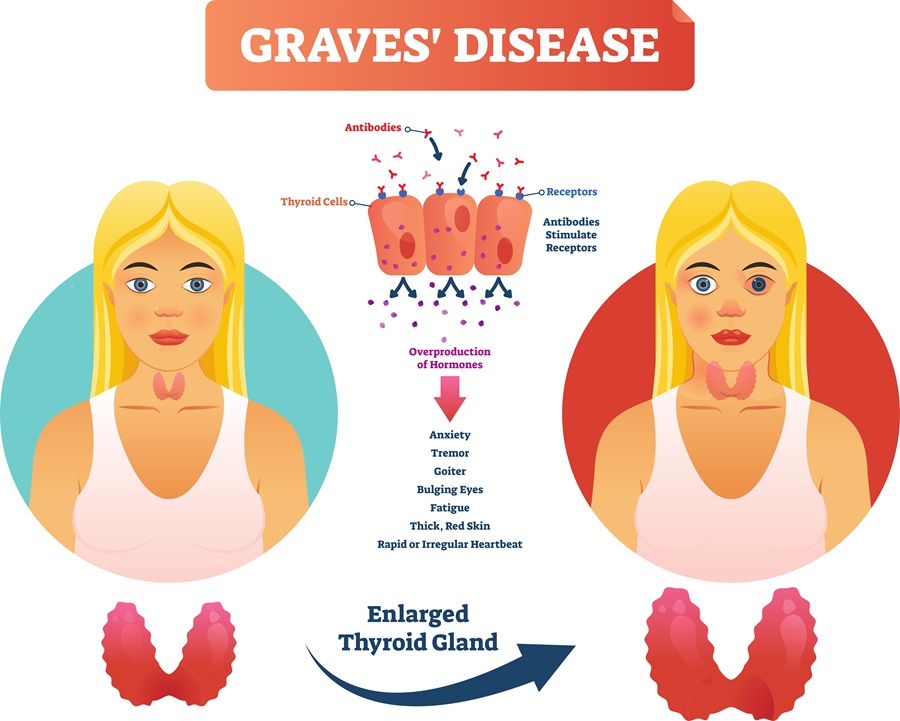
 Figure 1: Causes of Graves’ Disease
Figure 1: Causes of Graves’ Disease
In Graves’ disease, the immune system attacks the thyroid gland, producing more thyroid hormones than needed, which can speed up various body functions 2. Typically, headaches are not associated with Graves’ disease, and although some studies suggest that hyperthyroidism may cause headaches, the connection is still unclear 1.
However, a recent medical case study published in the scientific journal Cureus has revealed a new link between Graves’ disease and bilateral temporal headaches. This groundbreaking study focuses on a unique case of headaches associated with Graves’ disease 1.
Graves’ Disease: The Hidden Culprit
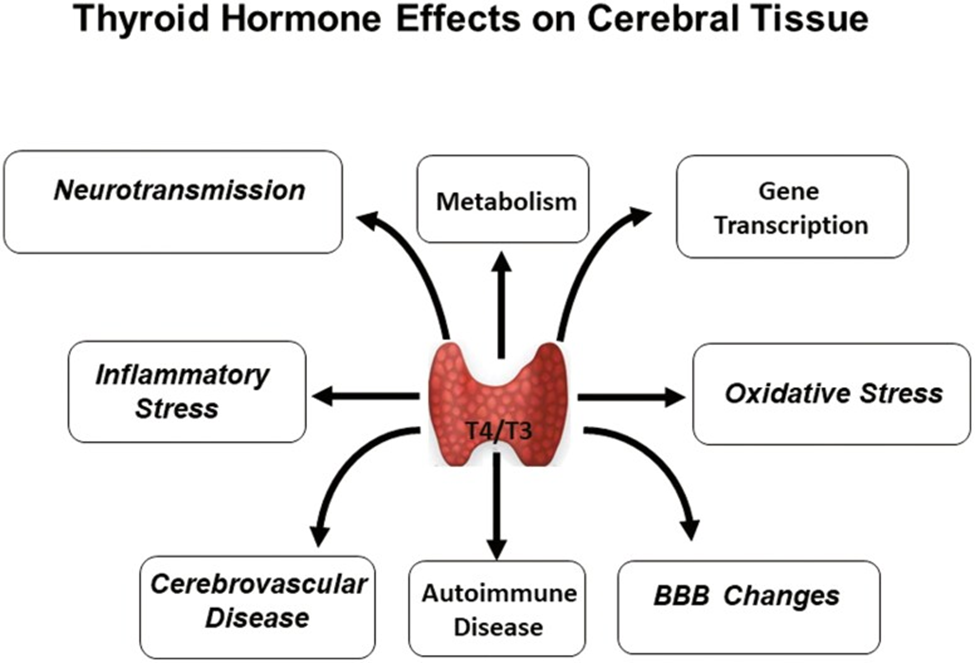
Figure 2: Thyroid hormone effects on cerebral tissue.
Source of Image: doi: 10.1210/jendso/bvab194
Headaches are a common complaint, with approximately 96% of people experiencing them at least once in their lifetime. According to a systematic review, headaches ranked the sixth highest patient-reported reason for visiting a primary health center. Although primary headache disorders are the most common differential diagnoses, clinicians must remember that secondary headache disorders remain an important cause of headaches 1. The International Classification of Headache Disorders (ICHD) categorizes secondary headache disorders into eight subtypes. Hyperthyroidism is not among the most common causes of secondary headaches, as per a study that included multiple centers in Asia, Africa, The Middle East, and Turkey 3. However, hyperthyroidism disorders like Graves’ disease are highly prevalent, with the prevalence of suspected cases in Jeddah, Saudi Arabia being 1.2%. A 10-year study in a Saudi Arabian hospital did not report headaches among the top 25 presentations of Graves’ disease. Furthermore, a literature review revealed only two cases where a headache was the presenting complaint of subacute thyroiditis and painless thyroiditis, respectively, and none where a headache was the presenting complaint of Graves’ disease 1.
Case Presentation 1
A 55-year-old male presented with intermittent headaches in the bilateral temporal area for the past two months. The severity of the headaches had increased over the last two weeks, lasting 30 minutes each time. The headaches were associated with blurred vision, left eye redness, pain, and lacrimation.
The patient appeared generally well with normal vitals. There was tenderness over the right temporal area, and the physician referred the patient to the Emergency Department as a case of query temporal arteritis due to the patient’s age and the area affected.
The patient underwent a blood test and a brain CT in the ER and was referred to Internal Medicine, Rheumatology, and Neurology. The brain CT showed no issues, and the labs were normal. The patient was given an outpatient appointment with Neurology and referred to Ophthalmology for suspected optic neuritis.
The patient was diagnosed with migraine headache and discharged with eye lubricants for the right eye. Later, thyroid panel results showed hyperthyroidism, and the patient was referred to the Endocrinology Department. A query for Graves’ ophthalmopathy was made, and a thyroid uptake scan showed diffuse, uniform iodine uptake at 6.5%, indicative of Graves’ disease. The patient was prescribed 5 milligrams of methimazole once daily, with an OPD follow-up appointment after one month. The patient reported complete subsidence of the headache since initiating the anti-thyroid medication.
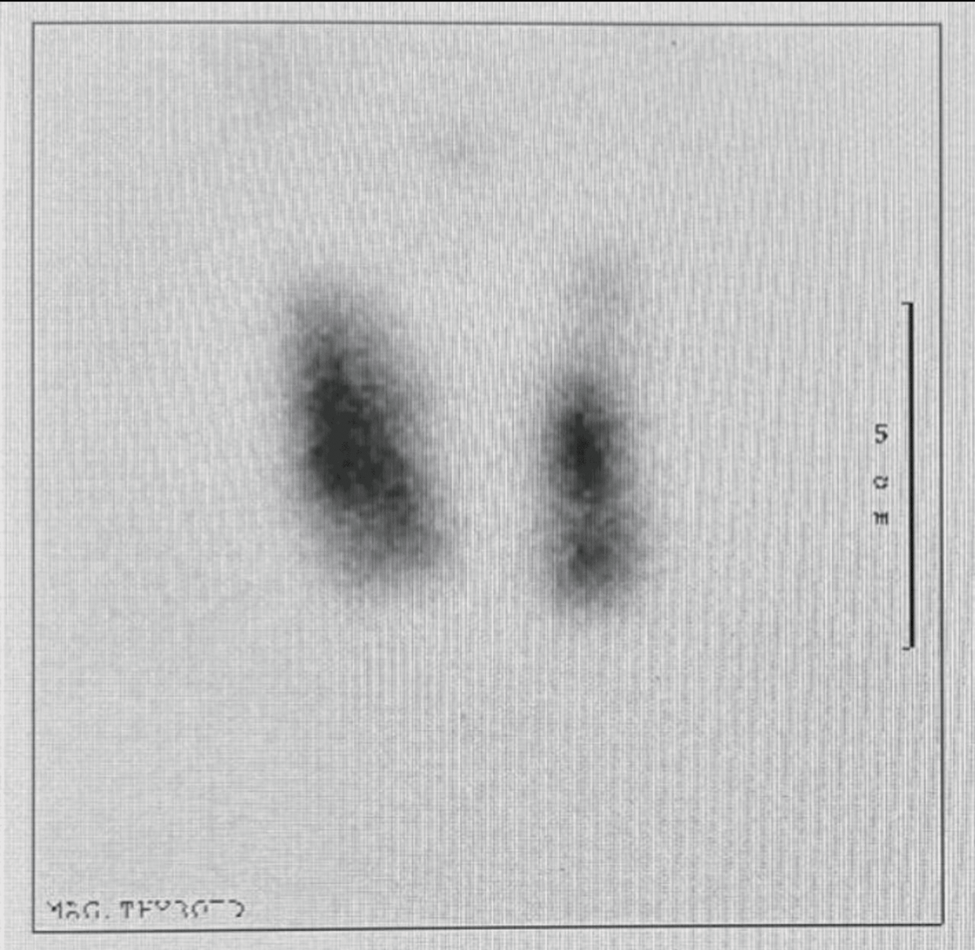
Figure 3: Thyroid scan and uptake
Discussion 1,2
Graves’ disease is the leading cause of hyperthyroidism, characterized by an autoimmune condition associated with circulating TSH receptor autoantibodies. It can cause headaches, but it is rarely considered in current approaches to isolated headaches. A thyroid panel is usually reserved for patients with the most commonly reported hyperthyroid symptoms. However, a recent case describes a rare occurrence of a headache as the presenting complaint of Graves’ disease. The patient experienced intermittent bilateral temporal pain headaches with associated symptoms such as blurred vision, left eye redness, pain, and lacrimation. The subtle right eyelid retraction observed by the ophthalmology team became a crucial clue in the diagnostic process. Ordering thyroid function tests and referring the patient to endocrinology based on the results were essential steps in taking further action in the management process. The pathophysiological mechanism explaining how hyperthyroidism could lead to headaches remains unclear, and more studies are needed to determine the relationship between thyroid hormone abnormalities and headaches.
Conclusion 1,2,3
Early detection and diagnosis are key to ensuring the best patient outcomes in healthcare. One condition that can sometimes present with atypical symptoms is Graves’ disease, a type of autoimmune disorder that affects the thyroid gland. While it is often associated with symptoms like weight loss, anxiety, and tremors, there are cases where the only symptom may be a recurring headache.
In a recent case study, a patient-reported experiencing headaches and subtle eyelid retraction but no other symptoms. After further investigation, it was discovered that the patient had Graves’ disease, a condition that can have serious long-term effects if left untreated. This case highlights the importance of considering thyroid-related disease as a potential cause of non-typical headaches, especially in patients who may not present with the more common symptoms associated with Graves’ disease.
Healthcare providers should be aware of this potential connection and consider performing a focused thyroid examination or investigation in patients with recurring headaches with no apparent cause. Early detection and diagnosis of Graves’ disease can help patients receive prompt treatment and avoid potential complications down the road.
References
- Alsabban AS, Bakri HM, Abduljabbar AZ, et al. Bilateral Temporal Headache As the Presenting Symptoms for a Case of Graves’ Disease. Cureus 15(12): e51344. December 30, 2023. doi:10.7759/cureus.51344
- Graves’ Disease [Internet]. National Institute of Diabetes and Digestive and Kidney Diseases. 2019. Available from: https://www.niddk.nih.gov/health-information/endocrine-diseases/graves-disease
- International Headache Society. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018 Jan;38(1):1–211. doi: 10.1177/0333102417738202
About Docquity
If you need more confidence and insights to boost careers in healthcare, expanding the network to other healthcare professionals to practice peer-to-peer learning might be the answer. One way to do it is by joining a social platform for healthcare professionals, such as Docquity.
Docquity is an AI-based state-of-the-art private & secure continual learning network of verified doctors, bringing you real-time knowledge from thousands of doctors worldwide. Today, Docquity has over 400,000 doctors spread across six countries in Asia. Meet experts and trusted peers across Asia where you can safely discuss clinical cases, get up-to-date insights from webinars and research journals, and earn CME/CPD credits through certified courses from Docquity Academy. All with the ease of a mobile app available on Android & iOS platforms!






