
Aarskog syndrome also recognized as Aarskog-Scott Syndrome, Facio-digital-genital Syndrome, or Faciogenital Dysplasia, is a rare genetic disorder linked to the X chromosome, primarily affecting males. It presents with distinctive facial, skeletal, and genital abnormalities. Herein, we present a case study involving a 15-year-old male who presented to a research institute with concerns about facial appearance. His medical history revealed consanguinity and a sibling with similar symptoms. A diagnosis of Aarskog syndrome was established through a comprehensive examination of the patient’s history, clinical assessment, and identification of characteristic radiographic features. Professional counseling was provided to explain the nature of the condition, and treatment options, including interventions for dental irregularities and congenital anomalies, were discussed and recommended.
Case Presentation of Aarskog-Scott Syndrome
1. Syndromes with Mild Manifestations: Conditions lacking severe medical issues or cognitive impairment might evade detection by unaware physicians.
2. Case Presentation – Aesthetic Complaint: Describing a 15-year-old male patient presenting with aesthetic concerns due to the lifelong absence of anterior teeth in both upper and lower jaws.
3. Absence of Dental History: Denying any history of tooth removal, exfoliation, or traumatic events in the anterior jaw region.
4. Familial Context: Noting his position as the second son of consanguineous parents, with an elder brother displaying short stature, missing teeth, and extra digits.
5. General Examination Findings: Observing short stature, adequate nourishment, and proper orientation in time, place, and person [Fig-1].
6. Physical Features: Noting sparse scalp hair and distinctive facial characteristics, including an enlarged nose, upper eyelid ptosis, and hypertrophied, everted lower lip [Fig-2].
7. Anthropometric Measurements: Recording a height of 1.32 meters, a weight of 46 kilograms, and normal vital signs [Fig-3].
8. Hexadactyly and Nail Abnormalities: Identifying six digits on each hand, accompanied by smaller-than-average nails [Fig-4].
9. Thumb and Finger Functionality: Noting the patient’s inability to adduct the thumb, index finger, and extra digit.
10. Lower Limb Abnormalities: Observing inward bowing of both lower limbs and the presence of six toes on each foot [Fig-5].

Figure 1: Short Stature

Figure 2: Sparse scalp hair

Figure 3: Large nose, droopy upper eyelids, hypertrophied and everted lower lip
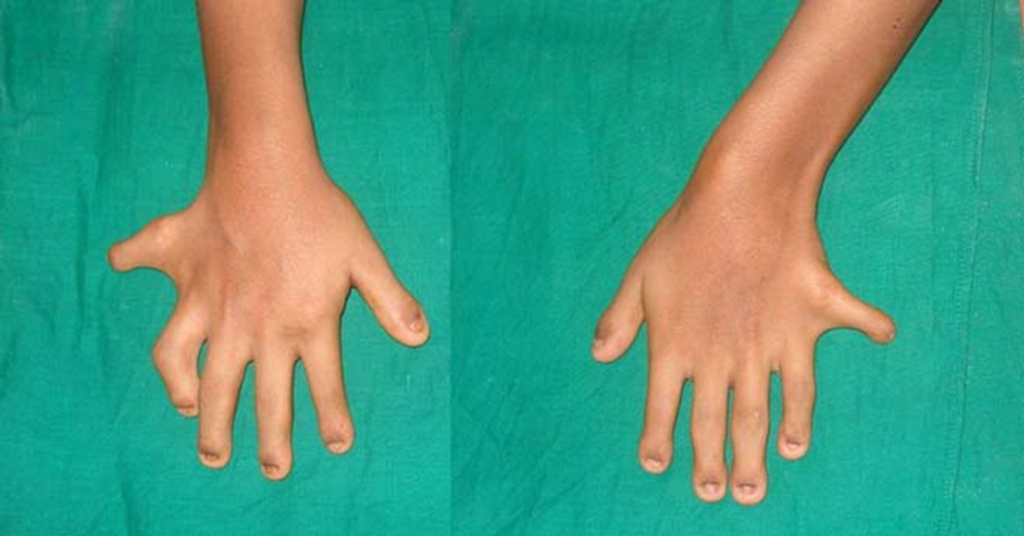
Figure 4: Extra finger on both hands, small nails

Figure 5: Bowing of legs and extra toes
11. Intra-Oral Examination Findings
- Noting an excessively large tongue covering the occlusal surface of the mandibular teeth.
- Identifying missing maxillary lateral incisors and all four mandibular incisors.
- Observing a high-arched palate with palatal positioning of second premolars [Fig-6].
12. Maxillary Central Incisors Abnormalities
- Describing macrodontic maxillary central incisors with altered morphology and diastema. [Fig-7].
- Noting the conical shape of all canines.
13. Soft Tissue and Ridge Abnormalities: Noticing soft tissue prominence and hyperplastic labial frenum in the edentulous ridge of the mandibular incisor region.
14. Provisional Diagnosis: Arriving at a provisional diagnosis of acrodental dysostoses based on history and clinical findings.
15. Differential Diagnoses Considered
- Considering Weyers’s accidental dysostosis due to dwarfism, postaxial polydactyly, and dysplastic teeth, but ruling it out due to the absence of reported systemic problems and normal vital signs.
- Mentioning Aarskog syndrome as a possibility, pending further examination of genital abnormalities.
- Excluding Leopard syndrome due to the absence of characteristic skin black macules and sensorineural deafness.

Figure 6: High-arched palate, missing lateral incisors, and palatally positioned premolars

Figure 7: Altered morphology of central incisors with midline diastema and missing mandibular central and lateral incisors
16. Clinical Findings
- Describing altered morphology and midline diastema in central incisors.
- Noting missing mandibular central and lateral incisors.
- Observing hyperplastic labial frenum and conical-shaped canines.
17. Diagnostic Investigations
- Conducting an Orthopantomograph (OPG) to confirm clinical observations regarding tooth number, shape, and position.
- Performing a hand wrist radiograph, revealing an extra digit and star-like pattern of the digits [Figure 8].

Figure 8: Star-like pattern of hand radiograph
18. Physician Examination
- Conducting further physical and clinical examinations by a general physician.
- Acknowledging the absence of cardiac problems but discovering unusual shawl-like tissue around the glans penis.
19. Presumptive Diagnosis: The most probable diagnosis is Aarskog syndrome due to the characteristic genital features.
20. Further Investigations
- Advising blood and genetic investigations to search for mutations in FGD1.
- Noting the patient’s reluctance for further investigations.
21. Patient Management: Providing prosthetic rehabilitation is the main concern of the patient, alongside explaining his condition.
Discussion
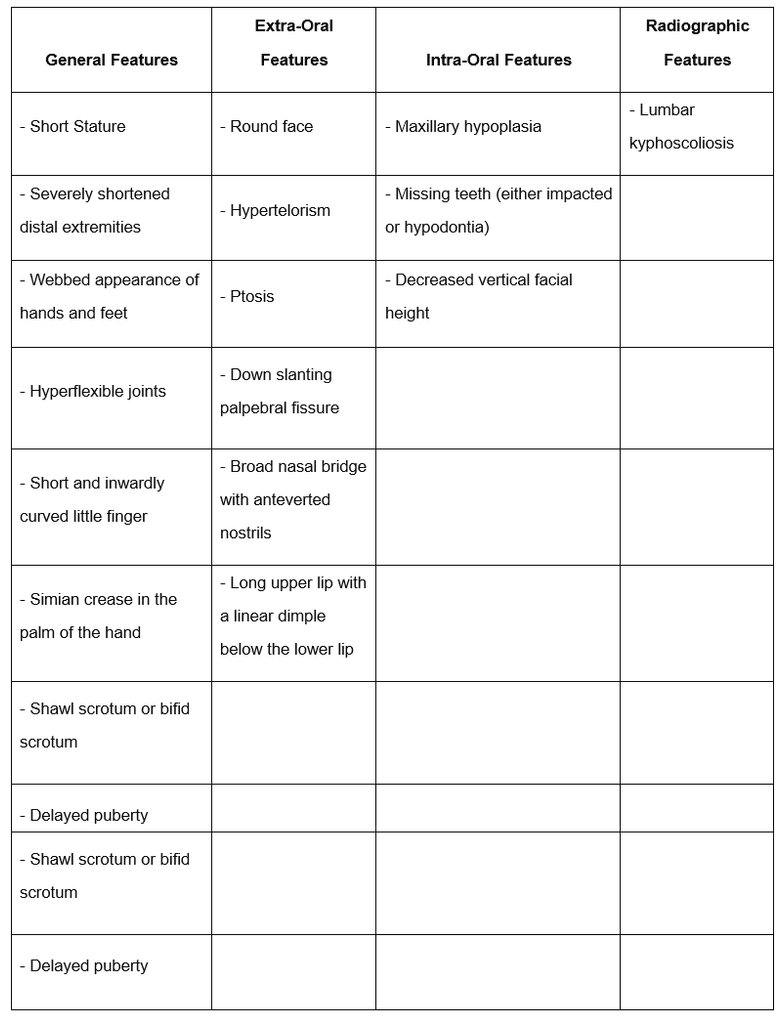
In 1970, Aarskog, in Norway, documented a syndrome characterized by short stature and specific facial, hand, foot, and genital anomalies in seven males spanning two generations of the same family [1]. The subsequent year, Scott reported a similar case [2], leading to its designation as Aarskog-Scott syndrome. This X-linked disorder results from mutations in the FGD1 gene, leading to full clinical manifestations in males, while female carriers typically exhibit minor symptoms, particularly in the face and hands [3]. Key features of Aarskog syndrome are outlined in [Table 1]. Population studies suggest an estimated prevalence of approximately 1 per one million individuals for Aarskog-Scott syndrome [4]. While most cases are diagnosed clinically, only 35 cases with molecular confirmation have been reported globally [Table 1][5].
Table 1: Typical Features of Aarskog Syndrome Reported in the Literature.
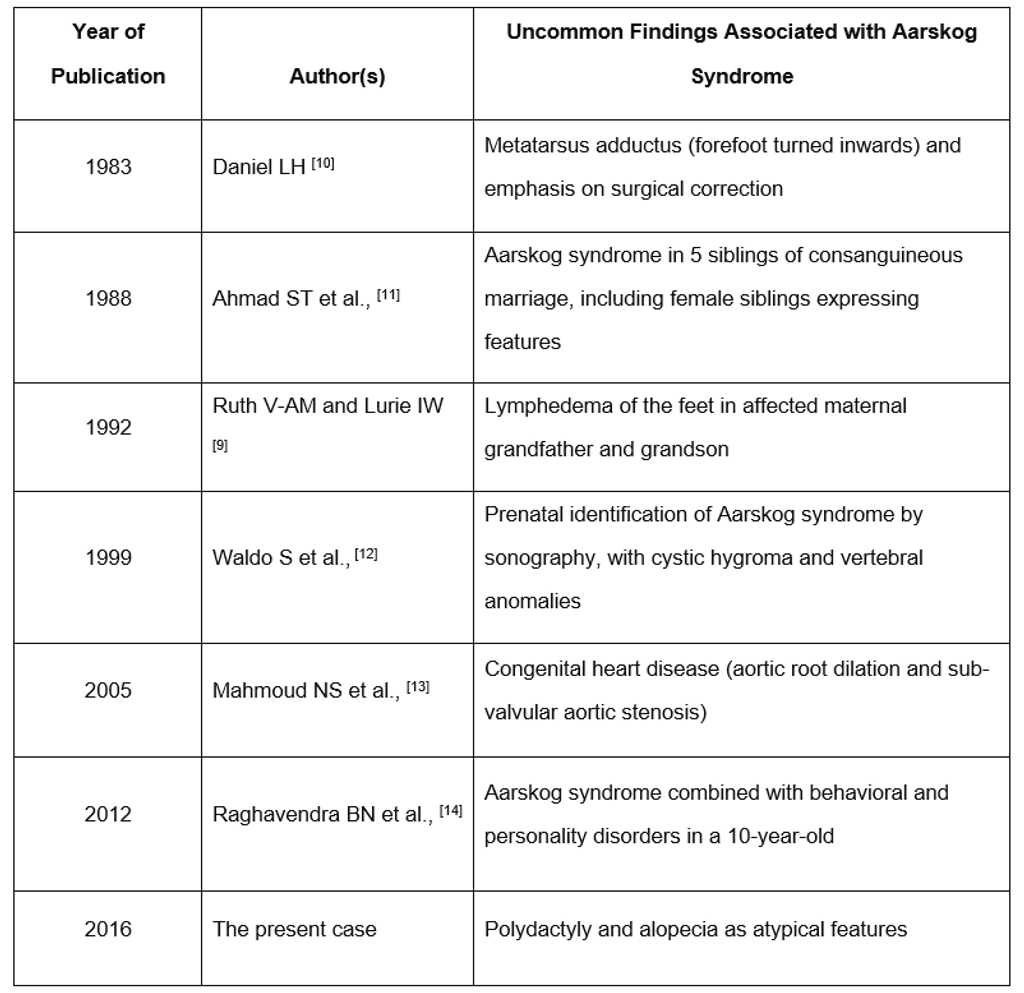
No targeted treatments exist for Aarskog syndrome. Surgical intervention may be required for certain features such as inguinal or umbilical hernias, cryptorchidism, and exceptionally severe craniofacial characteristics [15]. The literature documents atypical features linked with Aarskog syndrome, as outlined in [Table 2].
Table 2: Typical Features Associated with Aarskog Syndrome Reported in the Literature
Conclusion
Aarskog syndrome might go unnoticed because of its rare occurrence and limited awareness. The dental and orofacial features exhibit distinct characteristics crucial for diagnosing conditions like Aarskog syndrome. The diagnosis and treatment of such uncommon syndromes necessitate a collaborative effort involving pediatricians, orthopedic surgeons, dentists, and neuropsychiatrists.
References
- Ahmed A, Mufeed A, machamparambathu AK, Hasoon U. Identifying Aarskog Syndrome. J Clin of Diagn Res. 2016; 10(12): ZD09-ZD11. https://www.doi.org/10.7860/JCDR/2016/22180/8982
- Berry C, Cree J, Mann T, Aarskog’s syndrome Arch Dis Child 1980 55:706-10.
- Orrico A, Galli L, Faivre L, Clayton-Smith J, Azzarello-Burri SM, Hertz JM, Aarskog–Scott syndrome: Clinical update and report of nine novel mutations of the FGD1 gene Am J Med Genet A 2010 152:313-18.
- Moraes SG, Guerra-Junio G, Maciel-Guerra AT, Female counterpart of shawl scrotum in Aarskog-Scott syndrome International Braz J Urol 2006 32:459-61.
- Gorski JL, Estrada L, Changzhi H, Zhou L, Skeletal-specific expression of Fgd1 during bone formation and skeletal defects in facio-genital dysplasia (FGDY; Aarskog syndrome) Dev Dyn 2000 218:573-86.
- Orrico A, Galli L, Clayton-Smith J, Jean-Pierre F, Clinical utility gene card for Aarskog–Scott syndrome (faciogenital dysplasia) – update 2015 Eur J of Hum Genet 2015 23(4)
- Bozorgmehr B, Kariminejad A, Hadavi V, Kariminejad MH, Aarskog–Scott syndrome: Report of 7 cases and review of literature Genetics in the third millennium 2006 4:954-56.
- Jones KL, Smith’s recognizable patterns of human malformations 2006 6th edW.B. Saunders Company:134-35.
- Luciane QC, Maximiano T, Caroline D, Daniele PC, Ivana AV, Aarskog-Scott syndrome: A review and case report Int J Clin Pediatr Dent 2012 5(3):209-12.
- Ruth V-AM, Lurie I W, Atypical case of Aarskog syndrome J Med Genet 1992 29:349-50.
- Daniel LH, Metatarsus adductus in two brothers with Aarskog syndrome J Med Genet 1983 20(6):477
- Ahmad ST, Kamal KN, Sadika AA, Qasem AS, New autosomal recessive faciodigitogenital syndrome J Med Genet 1988 25:400-06.
- Waldo S, Victor D, Eleonora H, Mariana A, Prenatal sonographic diagnosis of Aarskog Syndrome J Ultrasound Med 1999 18:707-10.
- Mahmoud NS, Asif H, Chaudhari MP, Joel D, Case report – Congenital Aarskog syndrome with aortic root dilatation and sub-valvular aortic stenosis: Surgical management Interact Cardiovasc Thorac Surg 2005 4:47-48.
- Raghavendra BN, Ambika L, Bhogale GS, Apandurangi A, Mania with Aarskog-Scott Syndrome Indian Pediatr 2012 49:327-28.
- Orrico A, Galli L, Obregon MG, de Castro Perez MF, Falciani M, Sorrentino V, unusually severe expression of craniofacial features in Aarskog-Scott Síndrome due to a novel truncating variant of the FDG1 gene Am J Med Genet A 2007 143:58-63.
About Docquity
If you need more confidence and insights to boost careers in healthcare, expanding the network to other healthcare professionals to practice peer-to-peer learning might be the answer. One way to do it is by joining a social platform for healthcare professionals, such as Docquity.
Docquity is an AI-based state-of-the-art private & secure continual learning network of verified doctors, bringing you real-time knowledge from thousands of doctors worldwide. Today, Docquity has over 400,000 doctors spread across six countries in Asia. Meet experts and trusted peers across Asia where you can safely discuss clinical cases, get up-to-date insights from webinars and research journals, and earn CME/CPD credits through certified courses from Docquity Academy. All with the ease of a mobile app available on Android & iOS platforms!






