
Aquagenic Syringeal Acrokeratoderma (ASA), a rare condition that flares up after water exposure and fades shortly after drying, is typically seen in young women, primarily affecting the palms and occasionally the feet. We documented a unique case of a 40-year-old Asian man with a 13-year history of erythema and pale brown flattened papules on his hands, excluding the palms. His knees, elbows, buttocks, and ankles also displayed dark red macules and patches. Interestingly, his lesions worsened and became more persistent with exhaustion. Remarkably, significant improvement was achieved only with subcutaneous botulinum toxin injections at a concentration of 50 UI per 1 ml. Dermoscopy proved invaluable for diagnosis and follow-up.
Content Warning: This article contains explicit medical imagery. Viewer discretion is advised.
Aquagenic Syringeal Acrokeratoderma (ASA) is a rare and fleeting condition triggered by water exposure that disappears shortly after drying. It predominantly affects young women, mainly targeting the palms and, to a lesser extent, the feet [1].
Aquagenic Syringeal Acrokeratoderma (ASA) Case Presentation
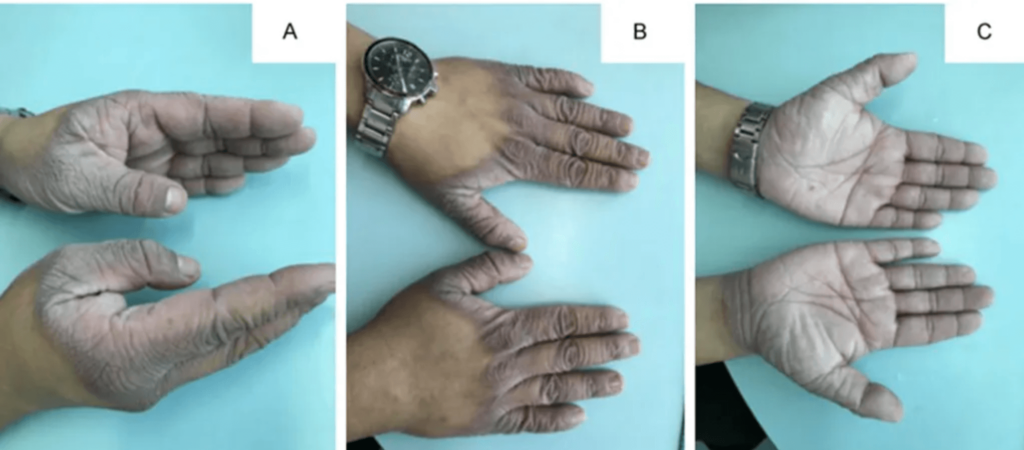
- Patient Profile: A 40-year-old Asian man with a 13-year history of erythema and pale brown flattened papules on his hands, sparing the palms (Figure 1A).
- Additional Affected Areas: Dark red macules and patches on knees, elbows, buttocks, and ankles (Figure 1E-1G).
- Symptoms After Water Immersion: Exaggerated wrinkling and eruption of white or translucent papules and plaques within 10 minutes of water exposure, sometimes peelable (Figure 1C).
- Seasonal Variation: Symptoms worsened in summer, remitted in winter, and subsided faster in drier environments.
- Exacerbation with Fatigue: Lesions became more severe and persistent when the patient felt exhausted.
- Impact of Sterile Gloves: Wearing sterile gloves for extended periods worsened the lesions.
- Childhood History: History of ichthyosis on the extended side of the lower legs during childhood.
- Family History: Father and elder sister have ichthyosis and dry skin.
- No Associated Conditions: No history of hyperhidrosis, thyroid disease, medication use, trauma, or atopic diseases.
- “Hands-in-the-Bucket” Sign: Significant, not visible until hands were exposed to water (Figure 1C) [2].
- Dermatoscopic Findings: Scattered gravel-like keratinized flat papules, milky white and translucent, partially fused into patches, with some whitish papules having central depression (Figure 1B, 1D).
- Sweat Chloride Test: The result was within the normal range.
- Diagnosis: ASA confirmed.
- Unsuccessful Treatments: Barrier cream, 20% aluminum chloride hexahydrate, 20% urea creams, salicylic acid preparations, and Traditional Chinese Medicine showed no improvement.

Figure 1: Aquagenic syringeal acrokeratoderma lesions. (A) Erythema and pale brown flattened papules on hands with involvement of opisthenars, dorsum of fingers, and wrist flexors. (B) Dermatoscopic examination revealed a yellow-white background with mild scales (Original magnifications ×20). (C) Translucent or whitish papules and plaques emerged as companions with mild maceration after immersing hands in water for 5 min. (D) Dermatoscopic examination revealed scattered gravel-like keratinized flat papules, milky white and translucent, partially fused into patches. Part of whitish papules with central depression. (Original magnifications ×20). The atypical lesions of aquagenic syringeal acrokeratoderma with the involvement of (E) elbows, (F) knees, (G) ankles, and (H) buttocks presented the same clinical features as hands when they were exposed to water.
- Botulinum Toxin (BoNT) Decision: Opted for BoNT infiltration.
- Injection Method: A 1-milliliter syringe and 33G 4 mm needles were used for subcutaneous injection.
- Dosage: Injected 50 units of BoNT into each lesion (concentration: 50 UI per 1 ml), spaced approximately 1 cm apart.
- Rapid Improvement: Significant improvement was observed within a week of BoNT injection [3].
- Sustained Results: No recurrence of symptoms within three months.
- Dermoscopy Findings: Normal dermatoscopic examination before and after water exposure.
Discussion
In 1996, English and McCollough uncovered a unique condition in two sisters who experienced transient and recurrent keratoderma on their palms solely after water contact [4]. Known as Aquagenic Syringeal Acrokeratoderma (ASA), this rare disorder predominantly affects young females, though occasional cases in males have been noted. Upon exposure to warm or hot water, the palms of ASA patients exhibit edematous, thickened, translucent to whitish, pebbly skin [5].
Atypical presentations involve the dorsal hands or the feet, while other sites are rarely affected. Symptoms can include itching, tightness, pain, or burning. Diagnosis hinges on clinical observation and the “hands in the bucket” test.
The exact cause of ASA is still a mystery. Still, factors like sweat-duct abnormalities, hyperkeratosis, an impaired stratum corneum barrier, hyperhidrosis, and elevated sweat salt concentration are believed to play a role [6]. There’s also a proposed link to cystic fibrosis, as seen in cases where lesions worsen and persist longer when the patient is exhausted.
It is crucial to differentiate ASA from similar conditions like Aquagenic Urticaria (AU) and Aquagenic Pruritus (AP). AU presents with itching, wheals, and erythema upon any water exposure, with symptoms vanishing within an hour and a positive water challenge test [7]. AP involves intense itching upon water contact without visible lesions. Understanding these nuances ensures accurate diagnosis and effective management of these rare conditions [8].
Despite no drug intake or abnormal sweat chloride test, the significant impact of BoNT injection hints at potential sweat gland irregularities. Dermoscopy, while underexplored in ASA, proved valuable for diagnosis and monitoring in our study.
ASA treatment options vary widely, including aluminum chloride hexahydrate, urea creams, aluminum lactate cream, Vaseline blends with salicylic acid, iontophoresis, and botulinum toxin (BoNT) injections [9]. Responses to these treatments are often unsatisfactory, highlighting the need for more effective therapies.
Despite lacking a standardized dosage, our experience suggests that BoNT injections can be beneficial. In this case, subcutaneous infusion of BoNT at 50 UI per 1 ml, spaced approximately 1 cm apart, showed promise in treating ASA with multiple atypical locations.
Conclusion
Showcases a unique ASA case in a clinical setting where fatigue exacerbated lesions across multiple locations. Treatment with BoNT injection proved effective, while dermatoscopy played a pivotal role in diagnosis and follow-up.
References
- Weng T, He J, Qi J, Yang Y. Atypical Multiple Aquagenic Syringeal Acrokeratoderma in a Patient Treatment with Botulinum Injection: A Case Report. Ann Clin Case Rep. 2023; 8:2536.
- Luo DQ. Aquagenic acrokeratoderma: A case with a family history and unusual involvements of the palms, soles, and the dorsum of fingers and toes. J Dermatol. 2011;38(6):612-5.
- Yan AC, Aasi SZ, Alms WJ, James WD, Heymann WR, Paller AS, et al. Aquagenic palmoplantar keratoderma. J Am Acad Dermatol. 2001;44(4):696-9.
- Garayar Cantero M, Delgado Mucientes C, Muñoz Fernández-Lomana C. Use of botulinum toxin in treating aquagenic keratoderma: One case report. Dermatol Ther. 2018;31(5):e12689.
- English JC 3rd, McCollough ML. Transient reactive papulotranslucent acrokeratoderma. J Am Acad Dermatol. 1996;34(4):686-7.
- Kutlubay Z, Engin B, Baglam S, Khatib R, Demirkesen C, Aydemir EH. Case report: Treatment failure in a case of aquagenic syringeal acrokeratoderma. J Cosmet Laser Ther. 2015;17(4):224-6.
- Luo DQ, Li Y, Huang YB, Wu LC, He DY. Aquagenic syringeal acrokeratoderma in an adult man: Case report and review of the literature. Clin Exp Dermatol. 2009;34(8): e907-9.
- Casale TB, Olsen JA, DelasAlas HC. Aquagenic urticaria. J Allergy Clin Immunol Pract. 2013;1(3):295-6.
- Lelonek E, Matusiak Ł, Wróbel T, Szepietowski JC. Aquagenic pruritus in polycythemia vera: A cross-sectional study. J Am Acad Dermatol. 2021;85(1):211-3.
- Pande P, Poonia K, Kaur J. Isolated aquagenic acrokeratoderma of dorsal hands. J Postgrad Med. 2021;67(3):184-5.
About Docquity
If you need more confidence and insights to boost careers in healthcare, expanding the network to other healthcare professionals to practice peer-to-peer learning might be the answer. One way to do it is by joining a social platform for healthcare professionals, such as Docquity.
Docquity is an AI-based state-of-the-art private & secure continual learning network of verified doctors, bringing you real-time knowledge from thousands of doctors worldwide. Today, Docquity has over 400,000 doctors spread across six countries in Asia. Meet experts and trusted peers across Asia where you can safely discuss clinical cases, get up-to-date insights from webinars and research journals, and earn CME/CPD credits through certified courses from Docquity Academy. All with the ease of a mobile app available on Android & iOS platforms!






