Pituitary adenomas represent a common subset of sellar region tumors, typically presenting with a diverse array of clinical manifestations. Among the myriad challenges these adenomas pose, calcification is rare and often raises suspicion of alternate diagnoses, such as craniopharyngiomas. Herein, we present a comprehensive case report detailing the clinical presentation, radiological findings, histopathological examination, and subsequent management of a 60-year-old woman with a known stellar mass. Despite initial radiological indications suggestive of a craniopharyngioma, meticulous analysis of calcification patterns and a thorough histopathological investigation confirmed the diagnosis of a pituitary adenoma. This case underscores the critical importance of detailed radiological evaluation and histopathological examination in accurately discerning between sellar lesions, thereby facilitating optimal patient management.
Introduction: Pituitary Adenoma
Pituitary adenomas represent a significant proportion of intracranial tumors, constituting approximately 5% to 20% of all central nervous system neoplasms. These adenomas arise from the adenohypophysis and can manifest with a wide spectrum of clinical features, including hormonal imbalances, visual disturbances, and headaches. While calcification is a relatively uncommon finding in pituitary adenomas, its presence can pose diagnostic challenges and necessitate consideration of alternative diagnoses, such as craniopharyngiomas. The distinction between these entities is paramount, as their management strategies differ significantly. We present a case highlighting the diagnostic complexities associated with sellar lesions and the critical role of comprehensive radiological and histopathological evaluations in establishing an accurate diagnosis.
Case Presentation
A 60-year-old female presented to the clinic with a progressive headache, worsening vision, and intermittent dizziness. The patient had a known history of a sellar mass diagnosed 15 years prior but had opted for medical management rather than surgical intervention. Physical examination revealed left temporal hemianopia and right superior quadrantanopia, consistent with optic nerve compression. Laboratory investigations demonstrated hyperprolactinemia, raising suspicion of a pituitary adenoma. Preoperative imaging, including non-contrast enhanced brain computed tomography (CT) and T2-weighted brain magnetic resonance imaging (MRI), revealed a large lobulated solid lesion filling the sella turcica with suprasellar extension. Notably, the lesion exhibited curvilinear peripheral thick nodular calcification, a finding typically associated with craniopharyngiomas. However, further histopathological analysis was warranted to confirm the diagnosis.
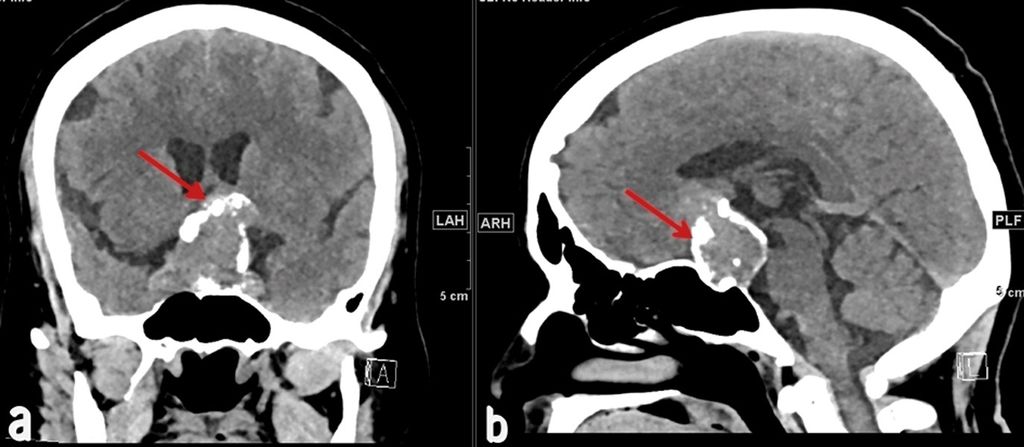
Figure 1: A pituitary mass with prominent curvilinear peripheral thick calcification is clearly depicted in both coronal (a) and sagittal (b) views of a non-contrast-enhanced brain CT scan, as indicated by the red arrows.
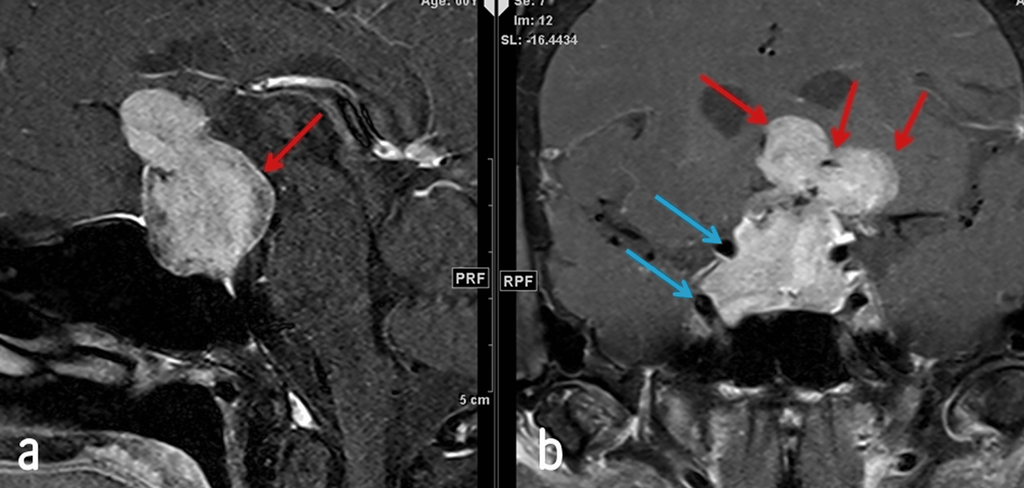
Figure 2: Enhanced T1-weighted fat-saturated brain MRI in both sagittal (a) and coronal (b) views reveals a mass compressing the hypothalamus and optic chiasm (red arrow). The internal carotid arteries are encased (blue arrows) without evidence of narrowing or occlusion. No cystic component is present.
Histopathological examination of the excised tissue revealed pituitary tissue composed of unevenly enlarged acini with moderate granular eosinophilic cytoplasm. Extensive calcification was evident within the lesion, corroborating the radiological findings. Immunohistochemistry studies demonstrated strong positivity for synaptophysin, with focal positivity for growth hormone, prolactin, follicle-stimulating hormone, and luteinizing hormone. However, the cytokeratin marker was negative, ruling out other differential diagnoses. The Ki-67 proliferative index showed a focal increase, indicative of tumor cell proliferation. Overall, the histopathological findings were consistent with a diagnosis of pituitary adenoma, confirming the initial clinical suspicion.
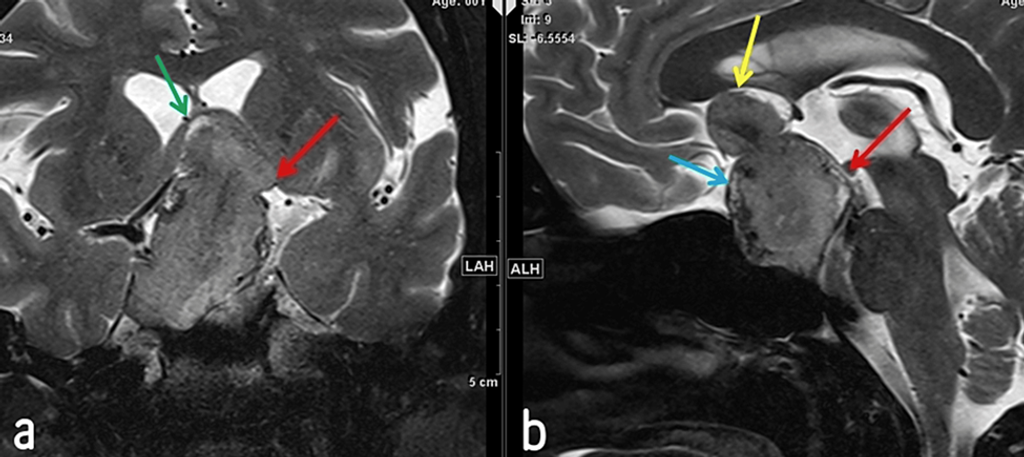
Figure 3: T2-weighted MRI in coronal (a) and sagittal (b) views shows a large sellar and suprasellar mass with intermediate signal intensity, elevating the third ventricle. The mass elevates the rostrum of the corpus callosum (yellow arrow) and abuts the mamillary bodies (red arrow). Peripheral calcification is visible (blue arrow), along with elevation of the fornix (green arrow).
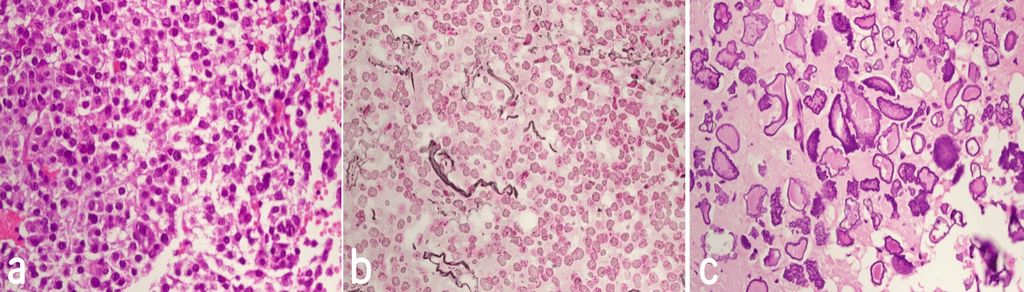
Figure 4: Photomicrograph of the tumor reveals round to polygonal cells with abundant eosinophilic to clear cytoplasm, forming acini (a). Reticulin stain shows partial loss of reticulin fibers (b), and areas with abundant calcification are visible (c).
Discussion
The differential diagnosis of sellar lesions encompasses many pathologies, including pituitary adenomas, craniopharyngiomas, meningiomas, and aneurysms. Radiological imaging is pivotal in distinguishing between these entities, with calcification patterns as a key diagnostic criterion. In the case presented, curvilinear peripheral thick nodular calcification initially raised suspicion of a craniopharyngioma, given its characteristic radiological appearance. However, histopathological examination confirmed a pituitary adenoma, highlighting the importance of corroborating radiological findings with histopathological analyses.
Intracranial calcifications indicate various pathological processes and can aid in narrowing down the differential diagnosis of sellar lesions. While craniopharyngiomas commonly exhibit calcification, pituitary adenomas rarely display such findings. The distinct patterns of calcification observed in these lesions, coupled with their characteristic radiological features, enable clinicians to differentiate between pituitary adenomas and craniopharyngiomas. Furthermore, immunohistochemistry studies can provide valuable insights into the tumor’s molecular characteristics, further refining the diagnostic approach.
Conclusion
In conclusion, the case presented underscores the diagnostic complexities associated with sellar lesions and the critical importance of comprehensive radiological and histopathological evaluations in establishing an accurate diagnosis. While calcified pituitary adenomas mimicking craniopharyngiomas pose significant diagnostic challenges, meticulous analysis of calcification patterns and histopathological features enables clinicians to differentiate between these entities and tailor management strategies accordingly. This case serves as a poignant reminder of the necessity for a multidisciplinary approach encompassing neuroimaging, histopathology, and clinical expertise in evaluating and managing sellar lesions.
Reference
Albadr FB, Alhatlani AH, Alhelal NS, et al. Calcified Pituitary Adenoma Mimicking Craniopharyngioma: A Case Report. Cureus. 2024 Feb 17. doi:10.7759/cureus.54352
About Docquity
If you need more confidence and insights to boost careers in healthcare, expanding the network to other healthcare professionals to practice peer-to-peer learning might be the answer. One way to do it is by joining a social platform for healthcare professionals, such as Docquity.
Docquity is an AI-based state-of-the-art private & secure continual learning network of verified doctors, bringing you real-time knowledge from thousands of doctors worldwide. Today, Docquity has over 400,000 doctors spread across six countries in Asia. Meet experts and trusted peers across Asia where you can safely discuss clinical cases, get up-to-date insights from webinars and research journals, and earn CME/CPD credits through certified courses from Docquity Academy. All with the ease of a mobile app available on Android & iOS platforms!






