

In recognition of Glaucoma Awareness Month in January, this article sheds light on the multifaceted challenges of glaucoma, a vision-threatening condition. The piece underscores the crucial role surgical interventions play in countering the impact of this formidable eye disorder by exploring the expertise of a skilled surgeon at Tsukazaki Hospital in Japan, who adeptly performs eight distinct types of glaucoma surgery. Understanding these surgical approaches becomes increasingly vital for individuals and healthcare practitioners as our global population ages. This is a timely reminder to prioritize eye health and stay informed about advancements in glaucoma treatment, ultimately fostering a proactive approach to maintaining clear vision and overall ocular well-being.
Glaucoma Surgery 1. Ab Interno Trabeculectomy
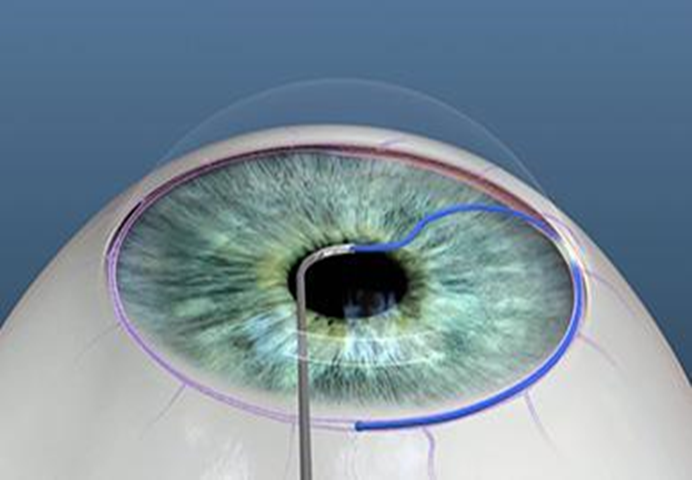
This minimally invasive procedure involves creating a small incision at the corneal ear side and using a micro hook to incise the trabecular meshwork. The surgeon skillfully navigates the anterior chamber to ensure proper drainage without leakage.
Procedure
An incision (1 mm) was made at two sites from the corneal ear side, and the anterior chamber was filled with a viscoelastic substance. Using a gonioscope to visualize the trabecular meshwork, an incision was made with a Tanito microhook, ranging from 120 to 180 degrees. The viscoelastic material was washed with a balanced salt solution (BSS). The procedure concluded after confirming the non-leakage of aqueous humor from the wound.
Glaucoma Surgery 2. Ab Externo Trabeculectomy
Employing a different approach, ab externo trabeculectomy utilizes a limbal conjunctival incision and a rectangular scleral flap. The surgeon identifies Schlemm’s canal, inserts a trabeculectome needle, and ensures efficient aqueous humor flow before meticulous suturing.
Procedure
- Sutures for corneal traction were placed using 9-0 silk to position the eyeball downward.
- A 7-mm limbal conjunctival incision was made.
- 2% lidocaine with epinephrine was applied to the sub-tenon for anesthesia and hemostasis.
- Hemostasis was ensured after creating space under Tenon’s capsule and the conjunctiva.
- A 4.5 mm × 3.5 mm rectangular scleral flap (half-thickness) was created near the limbus.
- Schlemm’s canal was identified at the flap’s edge, where a trabeculectome needle was inserted.
- After ensuring the needle’s placement inside Schlemm’s canal, it was removed and rotated toward the anterior chamber.
- Using 10-0 nylon (MANI, Utsunomiya, Japan), the scleral flap, followed by the conjunctiva, was sutured.
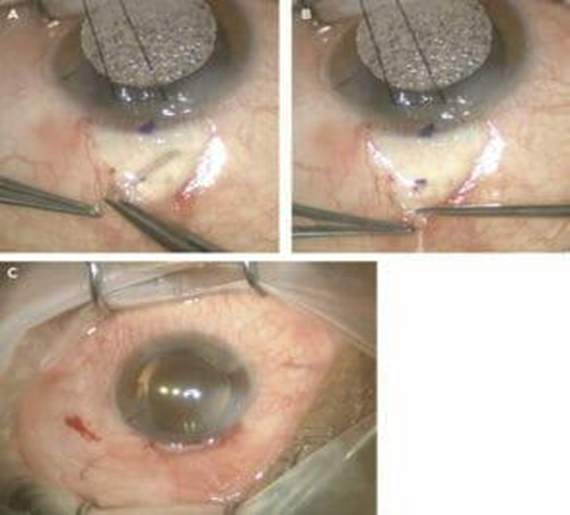
Glaucoma Surgery 3. Trabeculectomy
This well-established procedure involves creating a square scleral flap, applying mitomycin C for enhanced efficacy, and crafting a secondary flap for optimal aqueous humor drainage. The surgeon executes a meticulous scleral tunnel and peripheral iridectomy to complete the procedure.
Procedure
- 9-0 silk was used for corneal traction.
- A 7-mm limbal conjunctival incision was made.
- 2% lidocaine with epinephrine was applied to the sub-tenon for anesthesia and hemostasis.
- Hemostasis was ensured once a broad fornix view was achieved by creating space under Tenon’s capsule and the conjunctiva.
- A half-thickness 2.5 mm × 2.5 mm square scleral flap was created.
- 0.04% mitomycin C (MMC) was applied for three minutes using a neurosurgical pad sponge underneath Tenon’s capsule and the conjunctiva, then rinsed with 100 mL of saline water.
- A secondary 2.0 mm × 2.0 mm flap was crafted, and a scleral tunnel was initiated.
- Peripheral iridectomy was performed after forming a window in the anterior chamber using a V-lance and Kelly punch.
- The scleral flap was sutured using 10-0 nylon with four to five manually adjusted stitches to achieve an intraocular pressure of 10-15 mmHg.
- The procedure was concluded after suturing the conjunctiva with 10-0 nylon sutures and verifying the non-leakage of aqueous humor.
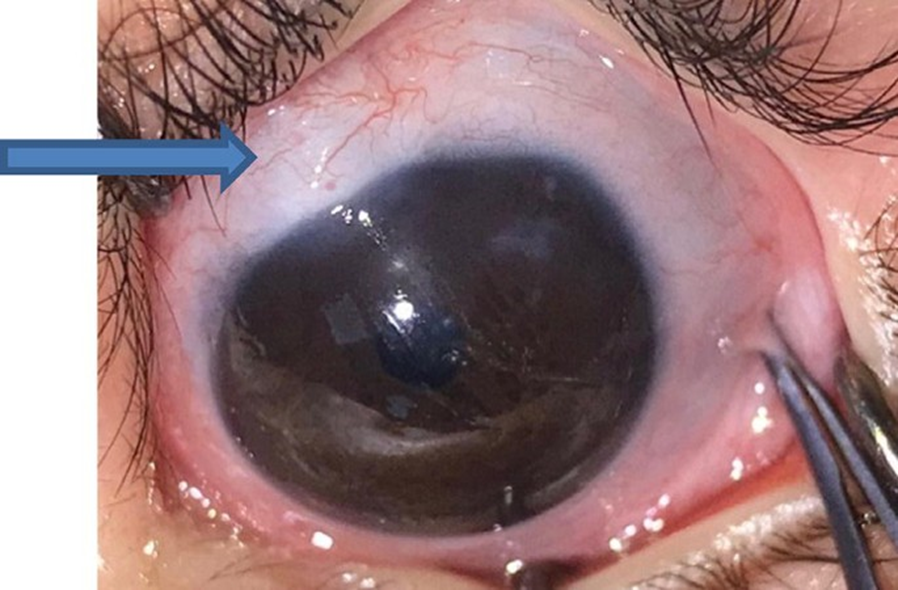
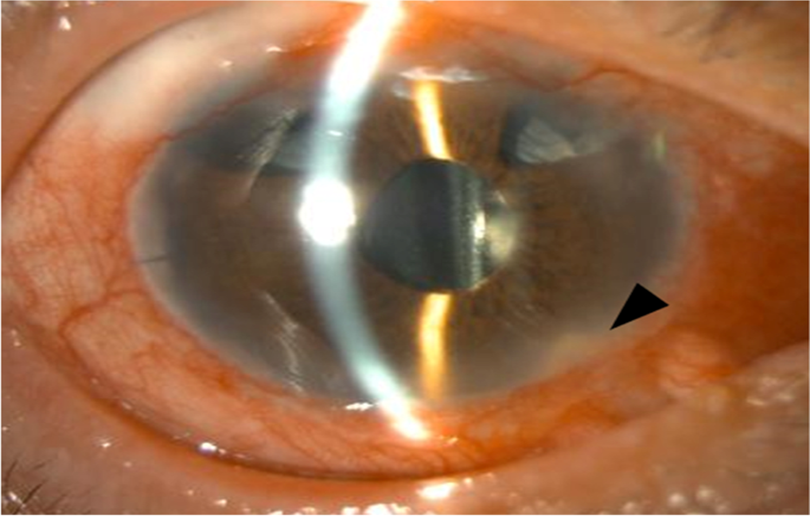
Glaucoma Surgery 4. Bleb Revision
A specialized technique, bleb revision involves incising the fornix conjunctiva and carefully addressing complications following previous trabeculectomy or EXPRESS procedures. Surgical finesse is crucial in ensuring minimal disruption and proper aqueous humor drainage.
Procedure
A fornix conjunctival incision was made, and 2% lidocaine with epinephrine was applied to the sub-tenon for anesthesia and hemostasis. The scleral flap was then identified. MMC was applied for three minutes and rinsed with 100 mL of saline water. A 1-mm side port was created in the cornea. The scleral flap was incised at its edge to verify aqueous humor flow. Intraocular pressure was evaluated, and the scleral flap was sutured with as few stitches as possible. The conjunctiva was closed with a continuous suture using 10-0 nylon. Non-leakage of aqueous humor was then confirmed.
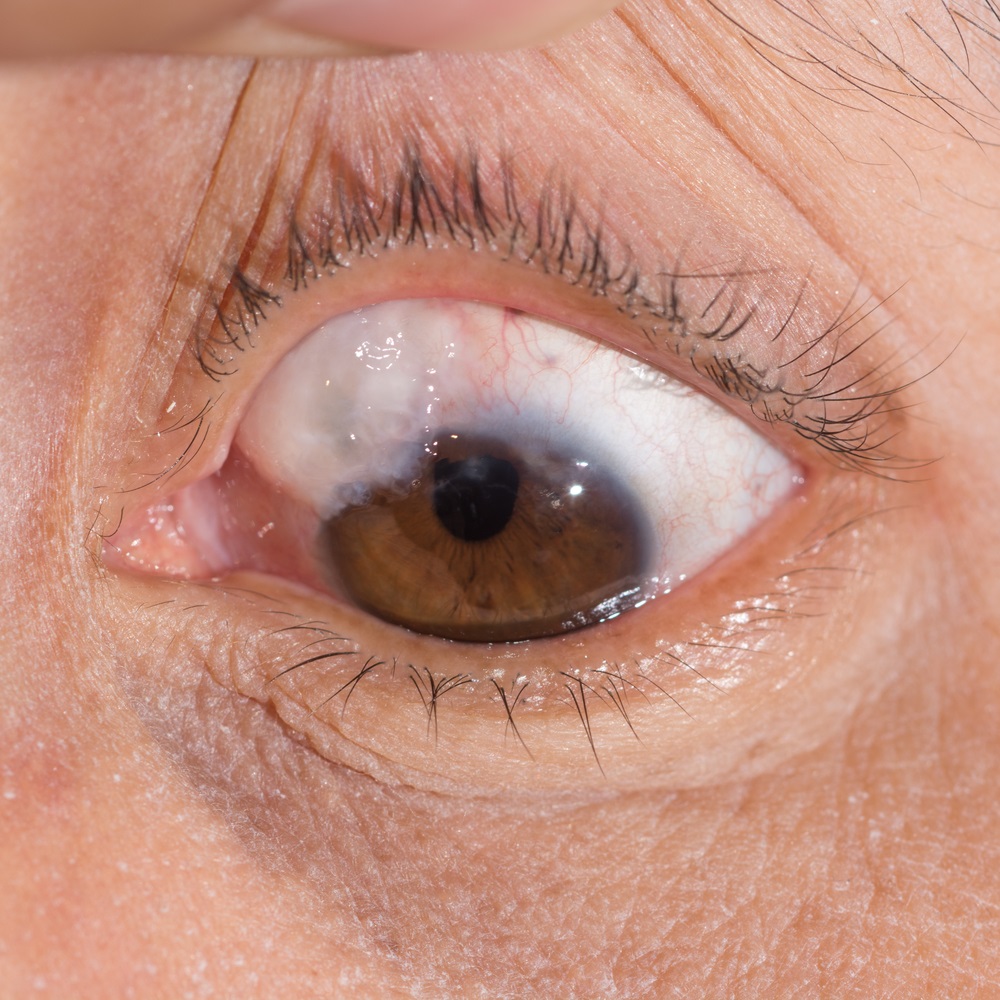
Glaucoma Surgery 5. EXPRESS
Similar to trabeculectomy, EXPRESS involves the application of mitomycin C, followed by the insertion of an EXPRESS device. The surgeon sutures the scleral flap, adjusting intraocular pressure to a target range, ensuring successful aqueous humor flow.
Procedure
Like trabeculectomy, MMC was applied, followed by conjunctival rinsing with 100 mL of saline water. Using a 25-G needle, an insertion into the anterior chamber was made parallel to the iris, after which the EXPRESS device was placed. Subsequently, the scleral flap was sutured with three to four stitches using 10-0 nylon, and intraocular pressure was manually adjusted to 10-15 mmHg by palpation. The procedure was concluded after suturing the conjunctiva with 10-0 nylon and verifying the non-leakage of aqueous humor.
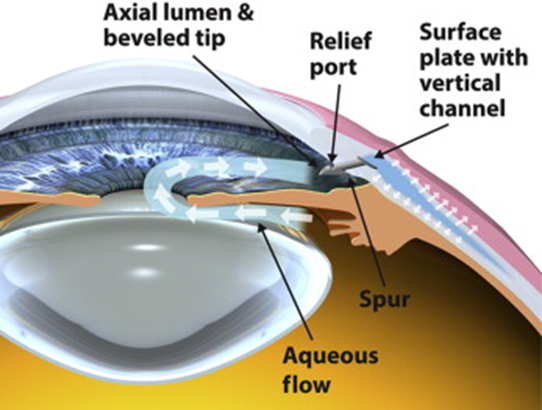
Glaucoma Surgery 6. PreserFlo
This technique employs meticulous steps, including eyeball retraction, sub-tenon anesthesia, and coagulation. Utilizing a 1-mm side port in the cornea, the surgeon inserts the PreserFlo device, confirming optimal flow before securing Tenon’s capsule and the conjunctiva.
Procedure
- The eyeball was retracted at the cornea using 7-0 silk sutures.
- Sub-Tenon anesthesia and hemostasis were achieved by applying 2% lidocaine with epinephrine.
- Space was created under Tenon’s capsule and the conjunctiva for broad observation. Coagulation was done.
- Using a neurosurgical pad, 0.04% MMC was applied for three minutes under Tenon’s capsule and the conjunctiva.
- Rinsing was done with approximately 200 mL of BSS.
- A 1-mm side port was created in the cornea.
- An incision was made 3.5 mm from the limbus using a dedicated knife, ensuring the tip entered the anterior chamber.
- PreserFlo was inserted, and BSS was injected from the port to confirm flow from PreserFlo.
- Tenon’s capsule and the conjunctiva were sutured over PreserFlo using 8-0 Vicryl.
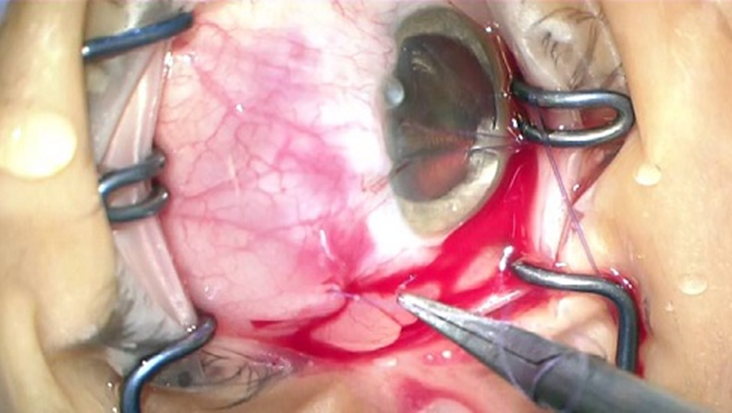
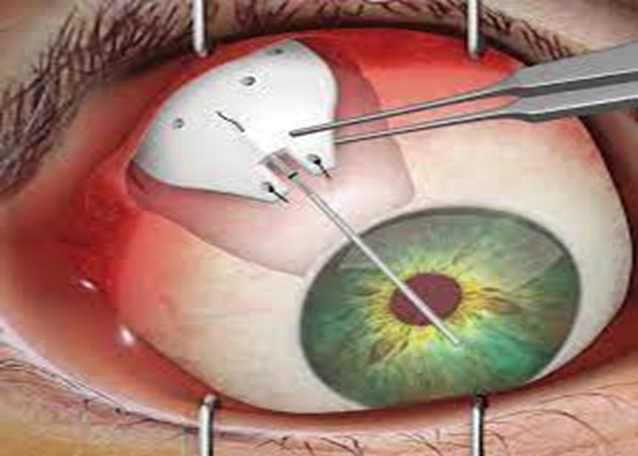
Glaucoma Surgery 7. Baerveldt
Incorporating conjunctival incision, extraocular muscle identification, and tube stenting, Baerveldt surgery aims to regulate aqueous humor outflow. The surgeon expertly places the tube through a puncture near the limbus, ensuring precise positioning and subsequent scleral fixation.
Procedure
- The conjunctiva was incised
- 2% lidocaine with epinephrine was applied to the sub-tenon for anesthesia and hemostasis
- Two extraocular muscles were identified
- BSS was injected into the implant to confirm the flow
- The tube was stented with 6-0 nylon and ligated with 8-0 Vicryl to block BSS outflow
- The plate was placed under the identified extraocular muscles
- A 23-G needle was used to puncture the eye 3 mm from the limbus
- The tube was inserted through the needle hole, and its placement in the target position was verified
- The tube was fixed to the sclera with 10-0 nylon
- A Sherwood slit was then created
- The tube and plate were covered with the preserved sclera and sutured with 10-0 nylon
- The conjunctiva was sutured with 8-0 Vicryl.
Glaucoma Surgery 8. Ahmed
This procedure involves conjunctival incision, extraocular muscle identification, and BSS injection to confirm implant flow. A 23-G needle puncture guides the tube insertion, with meticulous scleral anchoring using 10-0 nylon. The preserved sclera covers the tube and plate, ultimately securing the conjunctiva.
Procedure
- The conjunctiva was incised.
- 2% lidocaine with epinephrine was applied to the sub-tenon for anesthesia and hemostasis.
- Two extraocular muscles were identified.
- BSS was injected into the implant to confirm the flow before placing the plate under the muscles.
- A puncture was made 3 mm from the limbus using a 23-G needle, confirming the desired position.
- The tube was inserted through the needle hole, and its placement in the target position was verified.
- The tube was anchored to the sclera with 10-0 nylon.
- The tube and plate were covered with the preserved sclera and fixed in place using 10-0 nylon.
- The conjunctiva was sutured with 8-0 Vicryl.
Glaucoma Awareness Month: Conclusion
In unveiling the intricacies of eight distinct glaucoma surgeries, this exploration into a surgeon’s expertise during Glaucoma Awareness Month celebrates the current state of ophthalmology and envisions a future marked by innovation. The surgeon’s adeptness in Ab Interno Trabeculotomy, Ab Externo Trabeculectomy, Trabeculectomy, Bleb Revision, EXPRESS, PreserFlo, Baerveldt, and Ahmed highlights a commitment to tailored approaches in the battle against glaucoma. As the global population ages, these surgical nuances become increasingly critical, emphasizing the need for ongoing research, innovation, and proficiency to navigate the complexities of this vision-threatening condition. This exploration serves as a reminder of the collective responsibility to advance surgical finesse and technological innovation for a clearer future combating glaucoma.
Reference
Hiroyuki Wakuda, Shunsuke Nakakura, Tomohiro Shojo. Comparative Analysis of Surgical Durations and Fees Across Eight Types of Glaucoma Surgery Performed by a Single Surgeon. Cureus. 16(1): e51675. doi:10.7759/cureus.51675
About Docquity
If you need more confidence and insights to boost careers in healthcare, expanding the network to other healthcare professionals to practice peer-to-peer learning might be the answer. One way to do it is by joining a social platform for healthcare professionals, such as Docquity.
Docquity is an AI-based state-of-the-art private & secure continual learning network of verified doctors, bringing you real-time knowledge from thousands of doctors worldwide. Today, Docquity has over 400,000 doctors spread across six countries in Asia. Meet experts and trusted peers across Asia where you can safely discuss clinical cases, get up-to-date insights from webinars and research journals, and earn CME/CPD credits through certified courses from Docquity Academy. All with the ease of a mobile app available on Android & iOS platforms!






