Gallbladder volvulus is a rare condition predominantly observed in older women with abnormal anatomy, causing the gallbladder to twist freely on the mesentery, leading to ischemia and necrosis. Diagnosing this condition preoperatively is challenging due to its similarity to cholecystitis, often resulting in intraoperative identification. In our case, a 90-year-old woman was admitted to the hospital with an initial diagnosis of acute cholecystitis. Utilizing a robotic-assisted laparoscopic approach, entry into the abdomen was achieved. Inside, the gallbladder was found to be gangrenous, detached from the liver bed, and twisted on the cystic duct. Despite severe inflammatory changes and adhesions, the gallbladder was successfully resected without complications, and the patient was discharged on the fifth postoperative day.
Introduction
Gallbladder volvulus, a recognized yet rare condition, has been documented in approximately 500 reported cases 1. This condition manifests when the gallbladder twists around the mesentery, typically causing an acute abdomen, particularly in older adults. Diagnosis before surgery is infrequent due to inconclusive radiological findings, often leading to the initial assumption of acute cholecystitis until intraoperative confirmation. Given the potential for gallbladder ischemia and necrosis resulting from the entrapment of the cystic artery, urgent surgical intervention becomes necessary. Laparoscopic cholecystectomy stands as the primary treatment approach for gallbladder volvulus 2. The literature suggests that sole reliance on medical management, including antibiotics, percutaneous gallbladder drainage, and therapeutic endoscopy with endoscopic retrograde cholangiopancreatography (ERCP), demonstrates limited efficacy in the treatment of gallbladder volvulus 3,4.
Case Presentation1
A 90-year-old female sought medical attention from her primary care physician (PCP) due to two days of abdominal pain. Described as sharp, moderate severity, and persistent throughout the day, the pain was accompanied by nausea, diarrhea, and decreased appetite.
The patient denied experiencing vomiting, fever, dysuria, or chest pain and provided no specific factors that worsened or alleviated the discomfort. The patient’s medical history revealed essential hypertension, irritable bowel syndrome with diarrhea, chronic obstructive pulmonary disease, and dementia. Past surgical procedures included a left nephrectomy, tonsillectomy, and partial mastectomy.
Upon physical examination, the patient exhibited a distended abdomen, hypoactive bowel sounds, and tenderness in the right upper quadrant with mild guarding.
Laboratory studies conducted by the PCP encompassed a complete blood count (CBC), comprehensive metabolic panel (CMP), lipase, creatinine kinase (CK), C-reactive protein (CRP), and troponin.
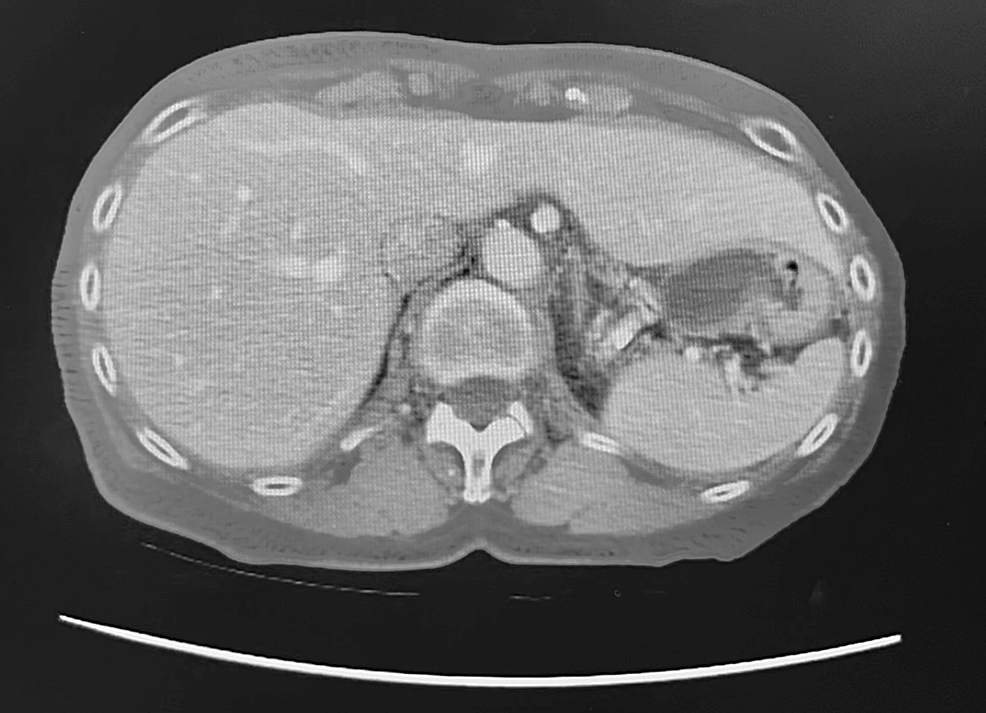
Results indicated leukocytosis with a left shift and elevated CRP (see Table 1). A computed tomography (CT) scan revealed a distended gallbladder in the pelvis with wall thickening (see Figures 1-3).
An abdominal ultrasound, though only the radiologic report was available, further depicted a dilated gallbladder with a small amount of sludge and possible pericholecystic fluid. Both imaging studies suggested the potential diagnosis of acute cholecystitis.
Subsequently, the patient was referred to a general surgeon to assess and consider treatment options.


Figure 1: CT showing empty gallbladder fossa

Figure 2: CT showing gallbladder in the right paracolic gutter/lateral to the right kidney

Figure 3: Alternative view of CT showing the gallbladder in the paracolic gutter/lateral to the right kidney
- Timeline
- Two days post-PCP visit.
- Four days pre-general surgeon appointment
- Emergency department presentation
- Patient’s Condition
- Persistent right upper quadrant pain
- Nausea
- Concurrent Findings
- Physical exam aligned with PCP documentation

- Physical exam aligned with PCP documentation
- Emergency Department Assessment
- Significant worsening in WBC and CRP levels (see Table 2)
- Decision-Making Factors
- Escalating leukocytosis
- Elevated CRP
- Advanced age of the patient
- Course of Action
- The decision to transfer to Amarillo, Texas, hospital for heightened care.
- Consultation
- General surgery was consulted upon the patient’s arrival.
- Diagnostic Process
- Cholecystitis was diagnosed after reviewing the patient’s history, prior evaluations, and relevant lab/imaging results.
- Treatment Plan
- Scheduled for robot-assisted laparoscopic cholecystectomy on the same day.

Figure 4: Intraoperative image demonstrating the inferior portion of the liver (red arrow) and the gallbladder nearly detached from the liver bed (black arrow) Figure 5: Intraoperative image demonstrating the gallbladder (black arrow) and the cystic duct (red arrow) that was previously twisted
Figure 5: Intraoperative image demonstrating the gallbladder (black arrow) and the cystic duct (red arrow) that was previously twisted
- Scheduled for robot-assisted laparoscopic cholecystectomy on the same day.
- Intraoperative Findings
- Severe inflammatory changes were observed around the gallbladder upon abdominal entry.
- Adhesions
- Duodenal and transverse colonic adhesions in the right upper quadrant obscured the gallbladder.
- Gallbladder Condition
- Gangrenous gallbladder
- Nearly detached from the liver bed
- Twisted on the cystic duct (see Figures 4, 5)
- Dissection Process
- Gallbladder and its vascular/biliary attachments dissected from surrounding structures
- Utilized electrocautery hook dissection
- Indocyanine green (ICG)-enhanced cholangiography aided in the dissection
- Intraoperative Course
- No complications observed, such as bleeding or bile leak
- Postoperative Transition
- The patient was transferred to the recovery room in stable condition
- Recovery Complications:
- Altered mental status and confusion
- Attributed to hospital-induced delirium
- Resolution
- Delirium resolved by the time of discharge
- Discharge Details
- Patient discharged on postoperative day five
- Post-Discharge Arrangements
- Transferred to a skilled nursing facility
- Follow-up & Outcome
- A follow-up appointment is scheduled in two weeks
- The patient did not return for the scheduled follow-up appointment
Discussion
Gallbladder volvulus, a rare condition predominantly impacting older adults, exhibits a four-to-one female-to-male ratio, with a median age of 77. Although its exact cause remains unclear, anatomical variants play a role, encompassing the absence of gallbladder mesentery, mesentery elongation with age, detachment from the liver bed, and fixation to a mobile hepatic lobe 1,2.
Events like atherosclerosis, abdominal trauma, or rapid weight loss trigger gallbladder torsion in predisposed individuals. Diagnosis proves challenging due to clinical, lab, and imaging similarities with acute cholecystitis. While ultrasound and CT scans provide suggestive features like distension, mobility, and twisted pedicle signs, Doppler ultrasound and HIDA scan contribute to the diagnosis 3,4.
Though the patient’s CT and ultrasound hinted at gallbladder issues, a definitive diagnosis remained elusive. Opting for robotic cholecystectomy, gaining popularity despite a preference for laparoscopic procedures, yielded excellent outcomes due to surgeon preference and institutional resources. Timely surgical intervention is crucial to minimize complications, with mortality staying below 5% when promptly managed 1,5.
Conclusion 1,2,3
In conclusion, maintaining awareness of gallbladder volvulus is crucial when assessing an elderly female patient with right upper quadrant pain and indications of acute cholecystitis in laboratory findings. Ultrasonography is the initial imaging method for diagnosis, with Doppler studies recommended in cases where suspicion of gallbladder volvulus is elevated. Given the unfavorable outcomes associated with conservative management, timely surgical intervention, either through laparoscopic or robotic cholecystectomy, is imperative to prevent potential complications such as sepsis, gallbladder rupture, and biliary peritonitis.
References
- Chugh J, Davis B, Sandoval J, et al. (November 08, 2023) Gallbladder Volvulus Masquerading as Acute Cholecystitis: A Case Report. Cureus 15(11): e48529. doi:10.7759/cureus.48529.
- Baig Z, Ljubojevic V, Christian F: The diagnostic dilemma of a gallbladder volvulus: an unusual case report and review of the literature. International Journal of Surgery Case Reports. 2021, 80:105614. 10.1016/j.ijscr.2021.01.108.
- Moser L, Joliat GR, Tabrizian P, et al.: Gallbladder volvulus. Hepatobiliary Surgery and Nutrition. 2021, 10:249-53. 10.21037.
- Cecire J, Sutherland A, Das KK: Gallbladder torsion masking as acalculus cholecystitis: a review of two cases including unsuccessful management with percutaneous cholecystostomy. Journal of Medical Cases. 2021, 12:223-5. 10.14740/jmc3683.
- Aharoni D, Hadas-Halpern I, Fisher D, Hiller N: Torsion of the fundus of gallbladder demonstrated on ultrasound and treated with ERCP. Abdominal Imaging. 2000, 25:269-71. 10.1007/s002610000031.
- Croce P, Licata S: Gallbladder volvulus: a case report. Journal of Medical Case Report. 2021, 15:494. 10.1186/s13256-021-03115-7.






