Background
The recent monkeypox outbreak is of global significance, and healthcare professionals and societies have enhanced their focus on its clinical manifestations.1 It is a viral, zoonotic disease with symptoms similar to that of smallpox, including fever, rashes, and swollen lymph nodes1. Multiple cases of monkeypox infection have been reported in men who engage in sexual activities with people of the same sex.2
Smallpox has previously been linked to myocarditis, or inflammation of the heart muscles.3 Furthermore, cardiac complications associated with the smallpox vaccine have strengthened this link.3 Similar associations have been proposed between the monkeypox virus and myocarditis.3
This article illustrates the case of a patient with monkeypox who developed acute myocarditis confirmed by cardiovascular magnetic resonance (CMR).
Case presentation
A 31-year-old man presented with discomfort, muscle pain, and fever, which had been persistent for the last five days.3 He also had multiple swollen lesions on his face, hands, and genital region.3 The skin lesions were used to collect swab samples and a monkeypox infection was confirmed following a positive PCR test.3
The patient returned to the emergency department three days later complaining of extreme chest tightness.3 He had several skin vesicles and pustules on his face, hands, legs, and genitalia, along with swelling of the foreskin and glans.3 One ulcerated lesion was present on his penis with lymphadenopathy in the left inguinal area.3 The patient was fully conscious and stable with no observed cardiopulmonary auscultation.3
Medical history
The patient has been taking medication for pre-exposure prophylaxis against human immunodeficiency virus (HIV) due to sexual risk exposure.3 He was receiving regular care at the Infectious Disease outpatient clinic.3
No history of adverse drug reactions, allergies, alcohol, or illegal drug use was recorded.3 He exhibited a few symptoms of a SARS-CoV-2 infection two months prior to this incidence.3
Examination
An electrocardiogram (ECG) indicated a sinus rhythm with abnormal ventricular repolarization, while a transthoracic echocardiogram (TTE) revealed preserved biventricular systolic function.3 The patient also had elevated levels of C-reactive protein, creatine phosphokinase, troponin I and a brain natriuretic peptide.3
A case of acute myocarditis was suspected, and the patient was admitted to an intensive care unit.3 CMR imaging after 24 hours revealed normal left ventricle (LV) wall thickness/volume and an LV ejection fraction (LVEF) of 56%.3
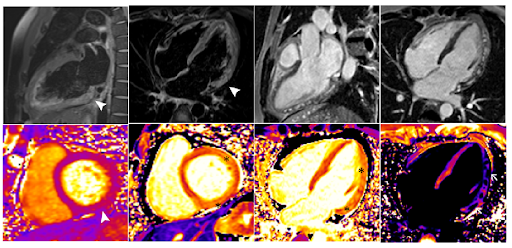
Figure 1: Cardiac magnetic resonance (CMR) imaging showing signs of myocardial edema and non-ischemic myocardial injury, suggestive of acute myocarditis.
Images revealed signs of myocardial edema, necrosis, and myocardial gadolinium accumulation with a non-ischemic pattern in the lateral wall (Figure 1).3 These observations were consistent with those of myocardial inflammation, indicating a case of acute myocarditis.3
Treatment approaches
The patient was provided adequate care and support. He was asked not to take any nonsteroidal anti-inflammatory drugs, particularly acetylsalicylic acid, and allowed to exercise with some limitations.3
Outcomes and follow-up
The patient made a full recovery within a week and was discharged thereafter.3 His cardiac enzymes were within normal limits with stable electric and hemodynamic stability. The skin lesions also began healing with tissue reepithelialization.3
Conclusion
Noninvasive diagnostic techniques such as CMR can be used to confirm the diagnosis of viral myocarditis.3 They can help healthcare professionals with clinical decisions and prevent invasive procedures.3 An improved understanding of acute myocarditis as a possible complication of monkeypox is useful for the close monitoring of affected patients and improving outcomes.3
Summary
- Myocarditis might be a possible complication of the monkeypox infection.
- It can be diagnosed based on clinical symptoms and imaging techniques like CMR.
- Additional research is needed to determine the pathological mechanism underlying monkeypox-linked myocarditis.
References
- Monkeypox. Who.int. 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/monkeypox
- Thornhill J, Barkati S, Walmsley S, Rockstroh J, Antinori A, Harrison L, et al. Monkeypox Virus Infection in Humans across 16 Countries — April–June 2022. New England Journal of Medicine. 2022;387(8):679-691.
- Pinho A, Braga M, Vasconcelos M, Oliveira C, Santos L, Guimarães A, Martins A, Chen-Xu J, Silva S, Macedo F. Acute Myocarditis – a new manifestation of Monkeypox infection? JACC: Case Reports. 2022.